
Page 9 - 2021 Sample Benefit Booklet
P. 9
MEDICAL COVERAGE
Kaiser Permanente
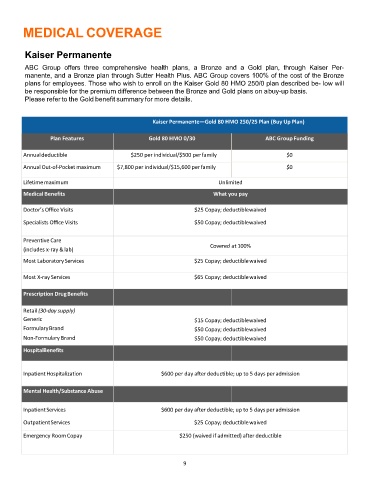
ABC Group offers three comprehensive health plans, a Bronze and a Gold plan, through Kaiser Per-
manente, and a Bronze plan through Sutter Health Plus. ABC Group covers 100% of the cost of the Bronze
plans for employees. Those who wish to enroll on the Kaiser Gold 80 HMO 250/0 plan described be- low will
be responsible for the premium difference between the Bronze and Gold plans on abuy-up basis.
Please refer to the Gold benefit summary for more details.
Kaiser Permanente—Gold 80 HMO 250/25 Plan (Buy Up Plan)
Plan Features Gold 80 HMO 0/30 ABC Group Funding
Annualdeductible $250 per individual/$500 perfamily $0
Annual Out‐of‐Pocket maximum $7,800 per individual/$15,600 perfamily $0
Lifetimemaximum Unlimited
Medical Benefits What you pay
Doctor’s Office Visits $25 Copay; deductiblewaived
Specialists Office Visits $50 Copay; deductiblewaived
Preventive Care
(includes x‐ray &lab) Covered at 100%
Most LaboratoryServices $25 Copay; deductiblewaived
Most X‐ray Services $65 Copay; deductiblewaived
Prescription DrugBenefits
Retail (30‐day supply)
Generic $15 Copay; deductiblewaived
FormularyBrand $50 Copay; deductiblewaived
Non‐Formulary Brand $50 Copay; deductiblewaived
HospitalBenefits
InpatientHospitalization $600 per day after deductible; up to 5 days peradmission
Mental Health/Substance Abuse
InpatientServices $600 per day after deductible; up to 5 days per admission
OutpatientServices $25 Copay; deductiblewaived
Emergency Room Copay $250 (waived if admitted) after deductible
9