
Page 199 - Atlas of Small Animal CT and MRI
P. 199
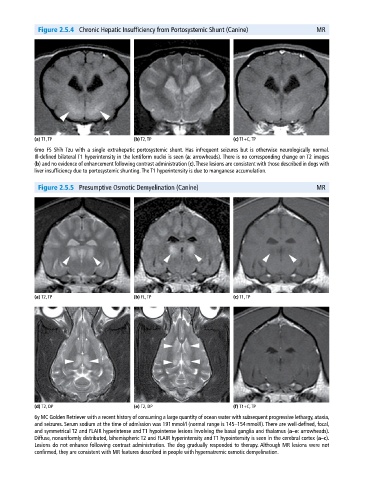
Figure 2.5.4 Chronic Hepatic Insufficiency from Portosystemic Shunt (Canine) MR
(a) T1, TP (b) T2, TP (c) T1+C, TP
6mo FS Shih Tzu with a single extrahepatic portosystemic shunt. Has infrequent seizures but is otherwise neurologically normal.
Ill‐defined bilateral T1 hyperintensity in the lentiform nuclei is seen (a: arrowheads). There is no corresponding change on T2 images
(b) and no evidence of enhancement following contrast administration (c). These lesions are consistent with those described in dogs with
liver insufficiency due to portosystemic shunting. The T1 hyperintensity is due to manganese accumulation.
Figure 2.5.5 Presumptive Osmotic Demyelination (Canine) MR
(a) T2, TP (b) FL, TP (c) T1, TP
(d) T2, DP (e) T2, DP (f) T1+C, TP
6y MC Golden Retriever with a recent history of consuming a large quantity of ocean water with subsequent progressive lethargy, ataxia,
and seizures. Serum sodium at the time of admission was 191 mmol/l (normal range is 145–154 mmol/l). There are well‐defined, focal,
and symmetrical T2 and FLAIR hyperintense and T1 hypointense lesions involving the basal ganglia and thalamus (a–e: arrowheads).
Diffuse, nonuniformly distributed, bihemispheric T2 and FLAIR hyperintensity and T1 hypointensity is seen in the cerebral cortex (a–c).
Lesions do not enhance following contrast administration. The dog gradually responded to therapy. Although MR lesions were not
confirmed, they are consistent with MR features described in people with hypernatremic osmotic demyelination.