
Page 3 - Luminex 2020 BLUE Triangles 12pg Guide w_Notices Final
P. 3
MEDICAL COVERAGE -
UNITEDHEALTHCARE
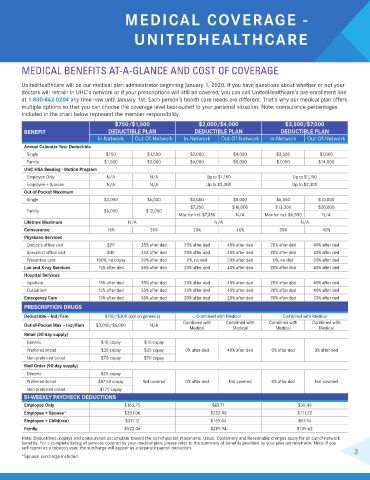
MEDICAL BENEFITS AT-A-GLANCE AND COST OF COVERAGE
UnitedHealthcare will be our medical plan administrator beginning January 1, 2020. If you have questions about whether or not your
doctors will remain in UHC’s network or if your prescriptions will still be covered, you can call UnitedHealthcare’s pre-enrollment line
at 1-800-842-0204 any time now until January 1st. Each person’s health care needs are different. That’s why our medical plan offers
multiple options so that you can choose the coverage level best-suited to your personal situation. Note: coinsurance percentages
included in the chart below represent the member responsibility.
$750/$1,500 $2,000/$4,000 $3,500/$7,000
BENEFIT DEDUCTIBLE PLAN DEDUCTIBLE PLAN DEDUCTIBLE PLAN
In-Network Out-Of-Network In-Network Out-Of-Network In-Network Out-Of-Network
Annual Calendar Year Deductible
Single $750 $1,500 $2,000 $4,000 $3,500 $7,000
Family $1,500 $3,000 $4,000 $8,000 $7,000 $14,000
UHC HSA Seeding - Motion Program
Employee Only N/A N/A Up to $1,150 Up to $1,150
Employee + Spouse N/A N/A Up to $2,300 Up to $2,300
Out-of-Pocket Maximum
Single $3,000 $6,000 $4,000 $8,000 $6,550 $10,000
$7,350 $16,000 $13,300 $20,000
Family $6,000 $12,000
Max for ind. $7,350 N/A Max for ind. $6,550 N/A
Lifetime Maximum N/A N/A N/A
Coinsurance 15% 35% 20% 40% 20% 40%
Physician Services
Doctor’s office visit $20 35% after ded 20% after ded 40% after ded 20% after ded 40% after ded
Specialist office visit $40 35% after ded 20% after ded 40% after ded 20% after ded 40% after ded
Preventive care 100%, no copay 20% after ded 0%, no ded 20% after ded 0%, no ded 20% after ded
Lab and X-ray Services 15% after ded 35% after ded 20% after ded 40% after ded 20% after ded 40% after ded
Hospital Services
Inpatient 15% after ded 35% after ded 20% after ded 40% after ded 20% after ded 40% after ded
Outpatient 15% after ded 35% after ded 20% after ded 40% after ded 20% after ded 40% after ded
Emergency Care 15% after ded 35% after ded 20% after ded 20% after ded 20% after ded 20% after ded
PRESCRIPTION DRUGS
Deductible – Ind/Fam $100/$300 (not on generics) Combined with Medical Combined with Medical
Combined with Combined with Combined with Combined with
Out-of-Pocket Max – Ind/Fam $3,000/$6,000 N/A
Medical Medical Medical Medical
Retail (30-day supply)
Generic $10 copay $10 copay
Preferred brand $35 copay $35 copay 0% after ded 40% after ded 0% after ded 0% after ded
Non-preferred brand $70 copay $70 copay
Mail Order (90-day supply)
Generic $25 copay
Preferred brand $87.50 copay Not covered 0% after ded Not covered 0% after ded Not covered
Non-preferred brand $175 copay
BI-WEEKLY PAYCHECK DEDUCTIONS
Employee Only $163.75 $83.71 $30.49
Employee + Spouse* $391.06 $222.98 $111.22
Employee + Child(ren) $311.12 $159.04 $57.94
Family $522.06 $289.94 $135.62
Note: Deductibles, copays and coinsurance accumulate toward the out-of-pocket maximums. Usual, Customary and Reasonable charges apply for all out-of-network
benefits. For a complete listing of services covered by your medical plan, please refer to the summary of benefits provided by your plan administrator. Note: If you
self-report as a tobacco user, the surcharge will appear as a separate payroll deduction. 3
*Spousal surcharge included