
Page 6 - Muchmore Harrington Renewal Booklet 2020
P. 6
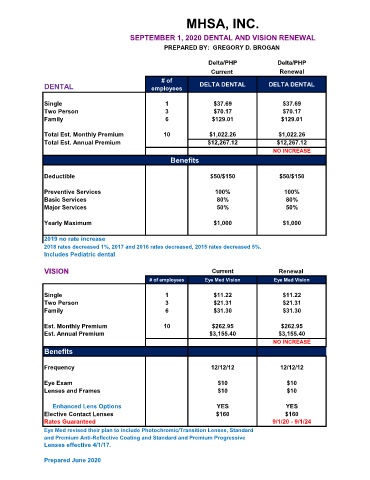
MHSA, INC.
SEPTEMBER 1, 2020 DENTAL AND VISION RENEWAL
PREPARED BY: GREGORY D. BROGAN
Delta/PHP Delta/PHP
Current Renewal
# of
DENTAL employees DELTA DENTAL DELTA DENTAL
Single 1 $37.69 $37.69
Two Person 3 $70.17 $70.17
Family 6 $129.01 $129.01
Total Est. Monthly Premium 10 $1,022.26 $1,022.26
Total Est. Annual Premium $12,267.12 $12,267.12
NO INCREASE
Benefits
Deductible $50/$150 $50/$150
Preventive Services 100% 100%
Basic Services 80% 80%
Major Services 50% 50%
Yearly Maximum $1,000 $1,000
2019 no rate increase
2018 rates decreased 1%, 2017 and 2016 rates decreased, 2015 rates decreased 5%.
Includes Pediatric dental
VISION Current Renewal
# of employees Eye Med Vision Eye Med Vision
Single 1 $11.22 $11.22
Two Person 3 $21.31 $21.31
Family 6 $31.30 $31.30
Est. Monthly Premium 10 $262.95 $262.95
Est. Annual Premium $3,155.40 $3,155.40
NO INCREASE
Benefits
Frequency 12/12/12 12/12/12
Eye Exam $10 $10
Lenses and Frames $10 $10
Enhanced Lens Options YES YES
Elective Contact Lenses $160 $160
Rates Guaranteed 9/1/20 - 9/1/24
Eye Med revised their plan to include Photochromic/Transition Lenses, Standard
and Premium Anti-Reflective Coating and Standard and Premium Progressive
Lenses effective 4/1/17.
Prepared June 2020