
Page 9 - QCHC.19 Employee Benefits
P. 9
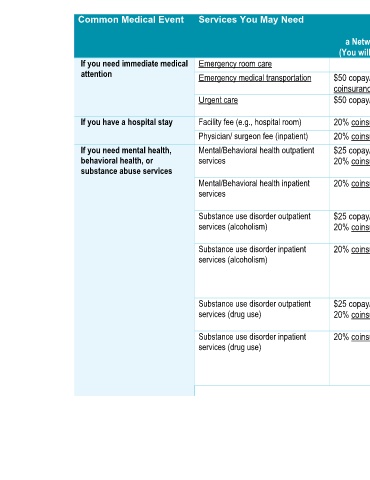
Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information a Non-Network Provider a Network Provider (You will pay the most) (You will pay the least) None $200 copay/visit, 20% coinsurance Emergency room care Emergency medical transportation None $50 copay/visit, 40% $50 copay/visit, 20% coinsurance coinsurance None $100 copay/visit, 40% $50 copay/visit Urgent care coinsurance Facility fee (e.g., hospital room) None 40% coinsurance 20% coinsurance None 40% coinsurance 20% coinsurance Physician/ surgeon fee (inpatient) (20 visits per benefit period, $50 copay/visit, deduc
Common Medical Event If you need immediate medical attention If you have a hospital stay If you need mental health, behavioral health, or substance abuse services