
Page 8 - COVID Assessment Centre TRAINING DOCUMENT
P. 8
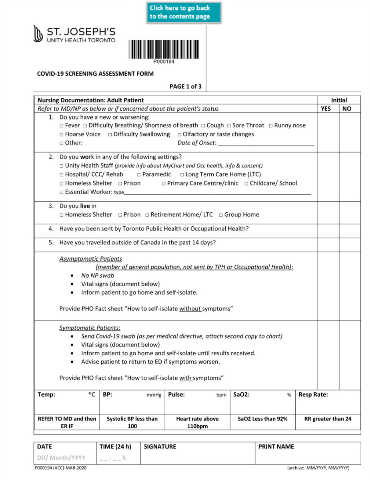
COVID-19 SCREENING ASSESSMENT FORM
PAGE 1 of 3
Nursing Documentation: Adult Patient Initial
Refer to MD/NP as below or if concerned about the patient’s status YES NO
1. Do you have a new or worsening:
□ Fever □ Difficulty Breathing/ Shortness of breath □ Cough □ Sore Throat □ Runny nose
□ Hoarse Voice □ Difficulty Swallowing □ Olfactory or taste changes
□ Other: Date of Onset: _____________________________
2. Do you work in any of the following settings?
□ Unity Health Staff (provide info about MyChart and Occ health, info & consent)
□ Hospital/ CCC/ Rehab □ Paramedic □ Long Term Care Home (LTC)
□ Homeless Shelter □ Prison □ Primary Care Centre/clinic □ Childcare/ School
□ Essential Worker: type_____________________________________________________________________
3. Do you live in
□ Homeless Shelter □ Prison □ Retirement Home/ LTC □ Group Home
4. Have you been sent by Toronto Public Health or Occupational Health?
5. Have you travelled outside of Canada in the past 14 days?
Asymptomatic Patients
(member of general population, not sent by TPH or Occupational Health):
• No NP swab
• Vital signs (document below)
• Inform patient to go home and self-isolate.
Provide PHO Fact sheet “How to self-isolate without symptoms”
Symptomatic Patients:
• Send Covid-19 swab (as per medical directive, attach second copy to chart)
• Vital signs (document below)
• Inform patient to go home and self-isolate until results received.
• Advise patient to return to ED if symptoms worsen.
Provide PHO Fact sheet “How to self-isolate with symptoms”
Temp: ®C BP: mmHg Pulse: bpm SaO2: % Resp Rate:
REFER TO MD and then Systolic BP less than Heart rate above SaO2 Less than 92% RR greater than 24
ER IF 100 110bpm
DATE TIME (24 h) SIGNATURE PRINT NAME
DD/ Month/YYYY _ _ : _ _ h
P000194 (ACC)-MAR-2020 (archive: MM/YYYY, MM/YYYY)