
Page 9 - COVID Assessment Centre TRAINING DOCUMENT
P. 9
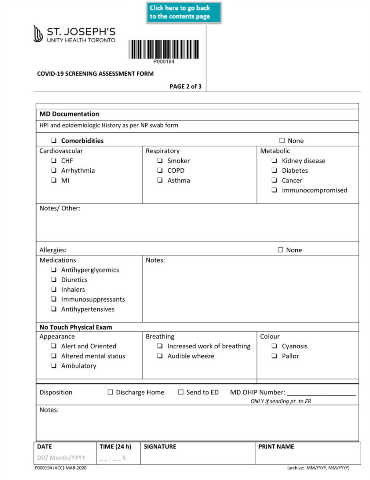
COVID-19 SCREENING ASSESSMENT FORM
PAGE 2 of 3
MD Documentation
HPI and epidemiologic History as per NP swab form
❏ Comorbidities □ None
Cardiovascular Respiratory Metabolic
❏ CHF ❏ Smoker ❏ Kidney disease
❏ Arrhythmia ❏ COPD ❏ Diabetes
❏ MI ❏ Asthma ❏ Cancer
❏ Immunocompromised
Notes/ Other:
Allergies: □ None
Medications Notes:
❏ Antihyperglycemics
❏ Diuretics
❏ Inhalers
❏ Immunosuppressants
❏ Antihypertensives
No Touch Physical Exam
Appearance Breathing Colour
❏ Alert and Oriented ❏ Increased work of breathing ❏ Cyanosis
❏ Altered mental status ❏ Audible wheeze ❏ Pallor
❏ Ambulatory
Disposition □ Discharge Home □ Send to ED MD OHIP Number: ___________________
ONLY If sending pt. to ER
Notes:
DATE TIME (24 h) SIGNATURE PRINT NAME
DD/ Month/YYYY _ _ : _ _ h
P000194 (ACC)-MAR-2020 (archive: MM/YYYY, MM/YYYY)