
Page 81 - Fluid, Electrolyte, and Acid-Base Disorders in Small Animal Practice
P. 81
Disorders of Sodium and Water: Hypernatremia and Hyponatremia 71
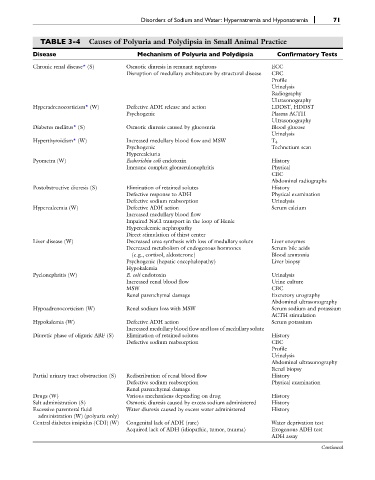
TABLE 3-4 Causes of Polyuria and Polydipsia in Small Animal Practice
Disease Mechanism of Polyuria and Polydipsia Confirmatory Tests
Chronic renal disease* (S) Osmotic diuresis in remnant nephrons ECC
Disruption of medullary architecture by structural disease CBC
Profile
Urinalysis
Radiography
Ultrasonography
Hyperadrenocorticism* (W) Defective ADH release and action LDDST, HDDST
Psychogenic Plasma ACTH
Ultrasonography
Diabetes mellitus* (S) Osmotic diuresis caused by glucosuria Blood glucose
Urinalysis
Hyperthyroidism* (W) Increased medullary blood flow and MSW T 4
Psychogenic Technetium scan
Hypercalciuria
Pyometra (W) Escherichia coli endotoxin History
Immune complex glomerulonephritis Physical
CBC
Abdominal radiographs
Postobstructive diuresis (S) Elimination of retained solutes History
Defective response to ADH Physical examination
Defective sodium reabsorption Urinalysis
Hypercalcemia (W) Defective ADH action Serum calcium
Increased medullary blood flow
Impaired NaCl transport in the loop of Henle
Hypercalcemic nephropathy
Direct stimulation of thirst center
Liver disease (W) Decreased urea synthesis with loss of medullary solute Liver enzymes
Decreased metabolism of endogenous hormones Serum bile acids
(e.g., cortisol, aldosterone) Blood ammonia
Psychogenic (hepatic encephalopathy) Liver biopsy
Hypokalemia
Pyelonephritis (W) E. coli endotoxin Urinalysis
Increased renal blood flow Urine culture
MSW CBC
Renal parenchymal damage Excretory urography
Abdominal ultrasonography
Hypoadrenocorticism (W) Renal sodium loss with MSW Serum sodium and potassium
ACTH stimulation
Hypokalemia (W) Defective ADH action Serum potassium
Increased medullary blood flow and loss of medullary solute
Diuretic phase of oliguric ARF (S) Elimination of retained solutes History
Defective sodium reabsorption CBC
Profile
Urinalysis
Abdominal ultrasonography
Renal biopsy
Partial urinary tract obstruction (S) Redistribution of renal blood flow History
Defective sodium reabsorption Physical examination
Renal parenchymal damage
Drugs (W) Various mechanisms depending on drug History
Salt administration (S) Osmotic diuresis caused by excess sodium administered History
Excessive parenteral fluid Water diuresis caused by excess water administered History
administration (W) (polyuria only)
Central diabetes insipidus (CDI) (W) Congenital lack of ADH (rare) Water deprivation test
Acquired lack of ADH (idiopathic, tumor, trauma) Exogenous ADH test
ADH assay
Continued