
Page 84 - Fluid, Electrolyte, and Acid-Base Disorders in Small Animal Practice
P. 84
74 ELECTROLYTE DISORDERS
Urine
specific 48 h
gravity (normal dogs)
2700 1.075
1.070
Normal, PPD w/o MSW
1.065 Normal
range
1.060
1.055
Urine osmolality (mOsm/kg) 1400 1.045 PPD w/ MSW
1.050
1800
1.040
1.035
Partial CDI
1.030
1100
1.025
Complete
700
1.020
CDI
500 1.015
NDI Isosthenuric
350 1.010 range
250 1.007
200 1.005
50 1.001
ADH administration
Time (hours)
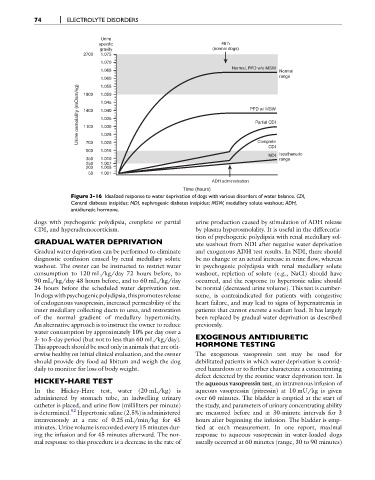
Figure 3-16 Idealized response to water deprivation of dogs with various disorders of water balance. CDI,
Central diabetes insipidus; NDI, nephrogenic diabetes insipidus; MSW, medullary solute washout; ADH,
antidiuretic hormone.
dogs with psychogenic polydipsia, complete or partial urine production caused by stimulation of ADH release
CDI, and hyperadrenocorticism. by plasma hyperosmolality. It is useful in the differentia-
tion of psychogenic polydipsia with renal medullary sol-
GRADUAL WATER DEPRIVATION ute washout from NDI after negative water deprivation
Gradual water deprivation can be performed to eliminate and exogenous ADH test results. In NDI, there should
diagnostic confusion caused by renal medullary solute be no change or an actual increase in urine flow, whereas
washout. The owner can be instructed to restrict water in psychogenic polydipsia with renal medullary solute
consumption to 120 mL/kg/day 72 hours before, to washout, repletion of solute (e.g., NaCl) should have
90 mL/kg/day 48 hours before, and to 60 mL/kg/day occurred, and the response to hypertonic saline should
24 hours before the scheduled water deprivation test. be normal (decreased urine volume). This test is cumber-
Indogswithpsychogenicpolydipsia,thispromotesrelease some, is contraindicated for patients with congestive
of endogenous vasopressin, increased permeability of the heart failure, and may lead to signs of hypernatremia in
inner medullary collecting ducts to urea, and restoration patients that cannot excrete a sodium load. It has largely
of the normal gradient of medullary hypertonicity. been replaced by gradual water deprivation as described
An alternative approach is to instruct the owner to reduce previously.
water consumption by approximately 10% per day over a
3- to 5-day period (but not to less than 60 mL/kg/day). EXOGENOUS ANTIDIURETIC
This approach should be used only in animals that are oth- HORMONE TESTING
erwise healthy on initial clinical evaluation, and the owner The exogenous vasopressin test may be used for
should provide dry food ad libitum and weigh the dog debilitated patients in which water deprivation is consid-
daily to monitor for loss of body weight. ered hazardous or to further characterize a concentrating
defect detected by the routine water deprivation test. In
HICKEY-HARE TEST the aqueous vasopressin test, an intravenous infusion of
In the Hickey-Hare test, water (20 mL/kg) is aqueous vasopressin (pitressin) at 10 mU/kg is given
administered by stomach tube, an indwelling urinary over 60 minutes. The bladder is emptied at the start of
catheter is placed, and urine flow (milliliters per minute) the study, and parameters of urinary concentrating ability
is determined. 92 Hypertonic saline (2.5%) is administered are measured before and at 30-minute intervals for 3
intravenously at a rate of 0.25 mL/min/kg for 45 hours after beginning the infusion. The bladder is emp-
minutes. Urine volume is recorded every 15 minutes dur- tied at each measurement. In one report, maximal
ing the infusion and for 45 minutes afterward. The nor- response to aqueous vasopressin in water-loaded dogs
mal response to this procedure is a decrease in the rate of usually occurred at 60 minutes (range, 30 to 90 minutes)