
Page 245 - Feline Cardiology
P. 245
250 Section F: Arrhythmias and Other Electrocardiographic Abnormalities
QRS
QRS
T
P P
T
A
QRS QRS
T P T P
P
Arrhythmias
B
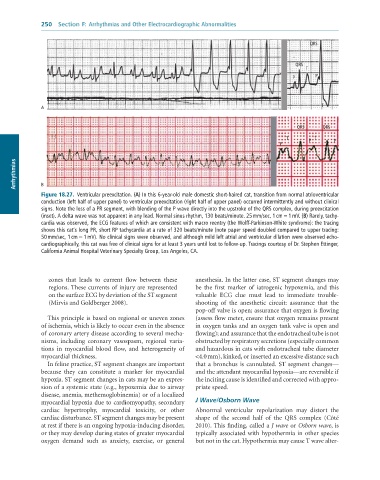
Figure 18.27. Ventricular preexcitation. (A) In this 6-year-old male domestic short-haired cat, transition from normal atrioventricular
conduction (left half of upper panel) to ventricular preexcitation (right half of upper panel) occurred intermittently and without clinical
signs. Note the loss of a PR segment, with blending of the P wave directly into the upstroke of the QRS complex, during preexcitation
(inset). A delta wave was not apparent in any lead. Normal sinus rhythm, 130 beats/minute. 25 mm/sec, 1 cm = 1 mV. (B) Rarely, tachy-
cardia was observed, the ECG features of which are consistent with macro reentry (the Wolff-Parkinson-White syndrome): the tracing
shows this cat’s long PR, short RP tachycardia at a rate of 320 beats/minute (note paper speed doubled compared to upper tracing:
50 mm/sec, 1 cm = 1 mV). No clinical signs were observed, and although mild left atrial and ventricular dilation were observed echo-
cardiographically, this cat was free of clinical signs for at least 3 years until lost to follow-up. Tracings courtesy of Dr. Stephen Ettinger,
California Animal Hospital Veterinary Specialty Group, Los Angeles, CA.
zones that leads to current flow between these anesthesia. In the latter case, ST segment changes may
regions. These currents of injury are represented be the first marker of iatrogenic hypoxemia, and this
on the surface ECG by deviation of the ST segment valuable ECG clue must lead to immediate trouble-
(Mirvis and Goldberger 2008). shooting of the anesthetic circuit: assurance that the
pop-off valve is open; assurance that oxygen is flowing
This principle is based on regional or uneven zones (assess flow meter, ensure that oxygen remains present
of ischemia, which is likely to occur even in the absence in oxygen tanks and an oxygen tank valve is open and
of coronary artery disease according to several mecha- flowing); and assurance that the endotracheal tube is not
nisms, including coronary vasospasm, regional varia- obstructed by respiratory secretions (especially common
tions in myocardial blood flow, and heterogeneity of and hazardous in cats with endotracheal tube diameter
myocardial thickness. <4.0 mm), kinked, or inserted an excessive distance such
In feline practice, ST segment changes are important that a bronchus is cannulated. ST segment changes—
because they can constitute a marker for myocardial and the attendant myocardial hypoxia—are reversible if
hypoxia. ST segment changes in cats may be an expres- the inciting cause is identified and corrected with appro-
sion of a systemic state (e.g., hypoxemia due to airway priate speed.
disease, anemia, methemoglobinemia) or of a localized
myocardial hypoxia due to cardiomyopathy, secondary J Wave/Osborn Wave
cardiac hypertrophy, myocardial toxicity, or other Abnormal ventricular repolarization may distort the
cardiac disturbance. ST segment changes may be present shape of the second half of the QRS complex (Côté
at rest if there is an ongoing hypoxia-inducing disorder, 2010). This finding, called a J wave or Osborn wave, is
or they may develop during states of greater myocardial typically associated with hypothermia in other species
oxygen demand such as anxiety, exercise, or general but not in the cat. Hypothermia may cause T wave alter-