
Page 243 - Feline Cardiology
P. 243
248 Section F: Arrhythmias and Other Electrocardiographic Abnormalities
T
T
QRS
QRS
+
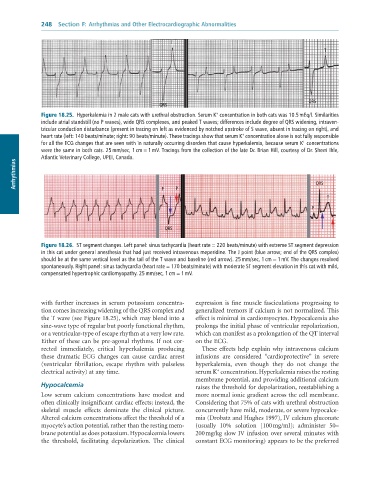
Figure 18.25. Hyperkalemia in 2 male cats with urethral obstruction. Serum K concentration in both cats was 10.5 mEq/l. Similarities
include atrial standstill (no P waves), wide QRS complexes, and peaked T waves; differences include degree of QRS widening, intraven-
tricular conduction disturbance (present in tracing on left as evidenced by notched upstroke of S wave, absent in tracing on right), and
+
heart rate (left: 140 beats/minute; right: 90 beats/minute). These tracings show that serum K concentration alone is not fully responsible
+
for all the ECG changes that are seen with in naturally occurring disorders that cause hyperkalemia, because serum K concentrations
were the same in both cats. 25 mm/sec, 1 cm = 1 mV. Tracings from the collection of the late Dr. Brian Hill, courtesy of Dr. Sherri Ihle,
Atlantic Veterinary College, UPEI, Canada.
Arrhythmias QRS
P
P
T
P
QRS
Figure 18.26. ST segment changes. Left panel: sinus tachycardia (heart rate = 220 beats/minute) with extreme ST segment depression
in this cat under general anesthesia that had just received intravenous meperidine. The J point (blue arrow; end of the QRS complex)
should be at the same vertical level as the tail of the T wave and baseline (red arrow). 25 mm/sec, 1 cm = 1 mV. The changes resolved
spontaneously. Right panel: sinus tachycardia (heart rate = 170 beats/minute) with moderate ST segment elevation in this cat with mild,
compensated hypertrophic cardiomyopathy. 25 mm/sec, 1 cm = 1 mV.
with further increases in serum potassium concentra- expression is fine muscle fasciculations progressing to
tion comes increasing widening of the QRS complex and generalized tremors if calcium is not normalized. This
the T wave (see Figure 18.25), which may blend into a effect is minimal in cardiomyocytes. Hypocalcemia also
sine-wave type of regular but poorly functional rhythm, prolongs the initial phase of ventricular repolarization,
or a ventricular-type of escape rhythm at a very low rate. which can manifest as a prolongation of the QT interval
Either of these can be pre-agonal rhythms. If not cor- on the ECG.
rected immediately, critical hyperkalemia producing These effects help explain why intravenous calcium
these dramatic ECG changes can cause cardiac arrest infusions are considered “cardioprotective” in severe
(ventricular fibrillation, escape rhythm with pulseless hyperkalemia, even though they do not change the
+
electrical activity) at any time. serum K concentration. Hyperkalemia raises the resting
membrane potential, and providing additional calcium
Hypocalcemia raises the threshold for depolarization, reestablishing a
Low serum calcium concentrations have modest and more normal ionic gradient across the cell membrane.
often clinically insignificant cardiac effects; instead, the Considering that 75% of cats with urethral obstruction
skeletal muscle effects dominate the clinical picture. concurrently have mild, moderate, or severe hypocalce-
Altered calcium concentrations affect the threshold of a mia (Drobatz and Hughes 1997), IV calcium gluconate
myocyte’s action potential, rather than the resting mem- (usually 10% solution [100 mg/ml]; administer 50–
brane potential as does potassium. Hypocalcemia lowers 200 mg/kg slow IV infusion over several minutes with
the threshold, facilitating depolarization. The clinical constant ECG monitoring) appears to be the preferred