
Page 242 - Feline Cardiology
P. 242
T T
R
A S
T T
R
P
S
B Arrhythmias
T T
C QS
R
T T
P
S
D
+
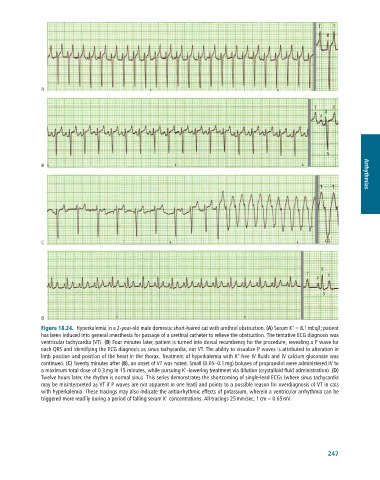
Figure 18.24. Hyperkalemia in a 2-year-old male domestic short-haired cat with urethral obstruction. (A) Serum K = 8.1 mEq/l; patient
has been induced into general anesthesia for passage of a urethral catheter to relieve the obstruction. The tentative ECG diagnosis was
ventricular tachycardia (VT). (B) Four minutes later, patient is turned into dorsal recumbency for the procedure, revealing a P wave for
each QRS and identifying the ECG diagnosis as sinus tachycardia, not VT. The ability to visualize P waves is attributed to alteration in
+
limb position and position of the heart in the thorax. Treatment of hyperkalemia with K -free IV fluids and IV calcium gluconate was
continued. (C) Twenty minutes after (B), an onset of VT was noted. Small (0.05–0.1 mg) boluses of propranolol were administered IV to
+
a maximum total dose of 0.3 mg in 15 minutes, while pursuing K -lowering treatment via dilution (crystalloid fluid administration). (D)
Twelve hours later, the rhythm is normal sinus. This series demonstrates the shortcoming of single-lead ECGs (where sinus tachycardia
may be misinterpreted as VT if P waves are not apparent in one lead) and points to a possible reason for overdiagnosis of VT in cats
with hyperkalemia. These tracings may also indicate the antiarrhythmic effects of potassium, wherein a ventricular arrhythmia can be
+
triggered more readily during a period of falling serum K concentrations. All tracings 25 mm/sec, 1 cm = 0.65 mV.
247