
Page 186 - Withrow and MacEwen's Small Animal Clinical Oncology, 6th Edition
P. 186
CHAPTER 10 Surgical Oncology 165
If one thinks about a given cancer as resembling a crab, Patients with recurrent cancer often have less normal tissue for
incomplete surgery removes the body of the crab but leaves the closure. Furthermore, changes in vascularity and local immune
legs behind. The “body” of most tumors is often quiescent and
responses may accompany local tumor recurrence.
VetBooks.ir hypoxic, whereas the leading edge of the tumor (legs) is the most and the surgeon should have all the necessary diagnostic informa-
Curative-intent surgery is best performed at the first surgery,
invasive and well vascularized. Thus subtotal removal may selec-
tively leave behind the most aggressive components of the tumor. tion to develop an appropriate treatment plan. Radiographs and
A
B
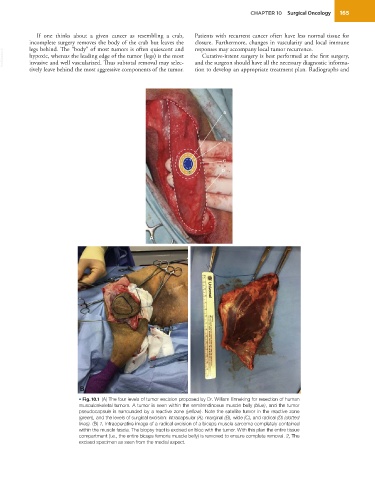
• Fig. 10.1 (A) The four levels of tumor excision proposed by Dr. William Enneking for resection of human
musculoskeletal tumors. A tumor is seen within the semitendinosus muscle belly (blue), and the tumor
pseudocapsule is surrounded by a reactive zone (yellow). Note the satellite tumor in the reactive zone
(green), and the levels of surgical excision: intracapsular (A), marginal (B), wide (C), and radical (D) (dotted
lines). (B) 1, Intraoperative image of a radical excision of a biceps muscle sarcoma completely contained
within the muscle fascia. The biopsy tract is excised en bloc with the tumor. With this plan the entire tissue
compartment (i.e., the entire biceps femoris muscle belly) is removed to ensure complete removal. 2, The
excised specimen as seen from the medial aspect.