
Page 145 - Manual of Equine Field Surgery
P. 145
Tracheotomy 141
but care must be taken to make sure the second
flange of the tube does not dissect subcutaneously.
This complication can be avoided by careful posi-
tioning and palpation of the tube after placement.
l
'i The self-retaining tracheotomy tubes have the
advantage of not completely relying on the tra-
cheotomy tube for an open airway. Therefore,
if the tube becomes clogged, there remains a
residual, albeit compromised, airway. Collapse or
"kinking" of the tube is also avoided with the use
of self-retaining tracheotomy tubes.
POSTOPERATIVE CARE
Tracheotomy -i....:,
incision site
~ostop~rative Care··
Tracheotomy tube Management: Trache-
otomy tubes require almost continuous mon-
itoring and management. The tubes and the
Figure 23-6 Incision site for tracheotomy. surrounding skin should be cleaned at least daily.
Scrubbing of the tracheotomy site should be
avoided. Exudate and blood clots should be
removed with a dry, sterile sponge, and the skin
surrounding the site should be cleaned. Extra
tubes should be immediately available.
Medications: Broad-spectrum antibiotics and
nonsteroidal antiinflammatory agents are generally
not necessary unless indicated for the treatment
of the underlying problem.
Other: After removal of the tracheotomy tube, the
wound is allowed to heal by second intention with
daily cleaning. Cleaning of the wound during
closure is performed at least once daily or as
needed with moistened gauze sponges. Petrola-
tum (Vaseline) is applied to the skin surrounding
the surgery site to prevent scalding from the anti-
cipated drainage. Healing is generaJ\y complete in
2 to 3 weeks.
I
~t;.,;f;,a.,,,__,
COMPLICATIONS
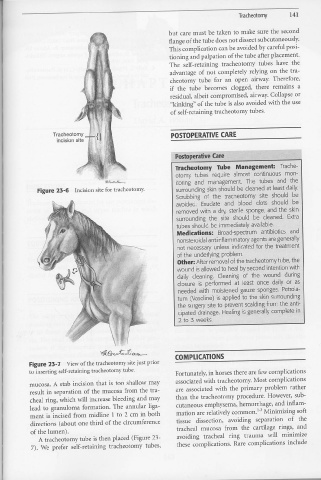
Figure 23-7 View of the tracheotomy site just prior
to inserting self-retaining tracheotomy tube. Fortunately, in horses there are few complications
associated with tracheotomy. Most complications
mucosa. A stab incision that is too shallow may
result in separation of the mucosa from the tra- are associated with the primary problem rather
cheal ring, which will increase bleeding and may than the tracheotomy procedure. However, sub-
lead to granuloma formation. The annular liga- cutaneous smphysema, hemorrhage, and inflam-
ment is incised from rnidline 1 to 2 cm in both mation are relatively common.!" Minimizing soft
directions (about 011e third of the circumference tissue dissection, avoiding separation of the
tracheal mucosa from the cartilage rings, and
of the lumen).
A tracheotomy tube is then placed (Figure 23- avoiding tracheal ring trauma will minimize
7). We prefer self-retaining tracheotomy tubes, these complications. Rare complications include