
Page 155 - Manual of Equine Field Surgery
P. 155
Dorsal Displacement of the Soft Palate 151
rated longitudinally the length of the incision (see
Figure 25-1). A self-retaining retractor is inserted
between the muscle bellies to expose the fascia
overlying the cricothyroid membrane. Sharp dis-
section is continued through the fascia. A small
vein is often present within the fascia that is tran-
sected. Bleeding is controlled with either hemo-
stats or electrocautery. The exposed cricothyroid
membrane is palpated. The caudal border of the
thyroid cartilage and the cranial border of the
cricoid cartilage are identified. The laryngotomy
I Mandibular inn. is then performed by placing the back of the
• ,'! • Cricothyroid
Thyroid . ..!,.-_ scalpel blade against the cricoid cartilage. A11
1~ membrane
cartilage~ initial stab incision is made into the laryngeal
. Laryngeal ventricle
lumen, and the incision is continued rostral to the
center of the thyroid cartilage. The self-retaining
retractors are then repositioned within the larynx.
The laryngeal lumen may be swabbed with a
Cricoid gauze sponge that has been soaked with local
cartilage
anesthetic solution (2o/o mepivacaine).
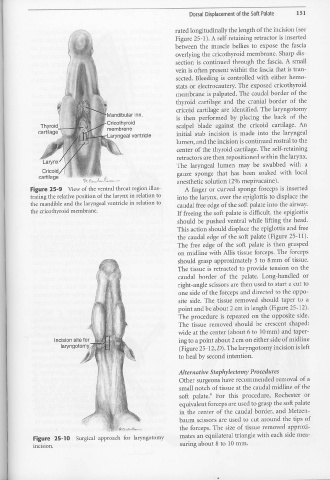
Figure 25-9 View of the ventral throat region illus- A finger or curved sponge forceps is inserted
trating the relative position of the larynx in relation to into the larynx, over the epiglottis to displace the
the mandible and the laryngeal ventricle in relation to caudal free edge of the soft palate into the airway.
the cricothyroid membrane. If freeing the soft palate is difficult, the epiglottis
should be pushed ventral while lifting the head.
This action should displace the epiglottis and free
the caudal edge of the soft palate (Figure 25-11).
The free edge of the soft palate is then grasped
011 midline with Allis tissue forceps. The forceps
should grasp approximately 5 to 8 mm of tissue.
The tissue is retracted to provide tension on the
caudal border of the palate. Long-handled or
right-angle scissors are then used to start a cut to
one side of the forceps and directed to the oppo-
site side. The tissue removed should taper to a
point and be about 2 cm in length (Pigure 25-12).
The procedure is repeated on the opposite side.
The tissue removed should be crescent shaped:
wide at the center (about 6 to 10 mm) and taper-
Incision site for ing to a point about 2 cm on either side of midline
larynqotorny, (Figure 25-12, D). The laryngotomy incision is left
to heal by second intention.
Alternative Staphylectorny Procedures
Other surgeons have recommended removal of a
l
small notch of tissue at the caudal midline of the
soft palate.6 For this procedure, Rochester or
•
equivalent forceps are used to grasp the soft palate
in the center of the caudal border, and Metzen-
baum scissors are used to cut around the tips of
the forceps. The size of tissue removed approxi-
mates an equilateral triangle with each side mea-
Figure 25-10 Surgical approach for laryngotomy
suring about 8 to 10 mm.
incision.
•