
Page 173 - Manual of Equine Field Surgery
P. 173
Eyelid Laceration Repair 169
COMPLICATIONS
The most frequent complication of eyelid lacera-
tion repair is wound dehiscence. This is most
commonly a result of single-layer closure, but it
may also occur as a result of devitalized wound
edges or excessive tension across the surgical site.
A B If wound dehiscence occurs, a second surgical
repair with debridement and suturing is recom-
mended to prevent eyelid margin defects and
to reduce the potential for corneal abrasion or
ulceration.
Some patients may develop a notch-like defect
of the eyelid. Such defects, if significant, can cause
abnormal tearfilm distribution, and corneal irri-
tation or ulceration. Minor defects of the eyelid
margin may be left alone if they do not adversely
affect the corneal surface; more significant defects,
C D however, require additional blepharoplastic tech-
~t?.r,v,f.<. ..:t~-- niques to correct or remove the defect. These
eyelid margin defects are most easily prevented by
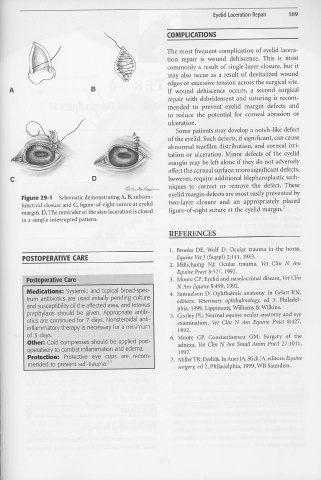
Figure 29-1 Schematic demonstrating A, B, subcon-
junctival closure and C, figure-of-eight suture at eyelid two-layer closure and a.11 appropriately placed
margin. D, The reminder of the skin laceration is closed figure-of-eight suture at the eyelid margin.2
in a simple interrupted pattern.
REFERENCES
1. Brooks DE, Wolf D: Ocular trauma in the horse,
I
POSTOPERATVE CARE Equine Vet J (Suppl) 2:141, 1983.
2. Millichamp NJ: Ocular trauma, Vet Clin N Am
Equine Pract 8:521, 1992.
. . .
Postoperative Care "' ··.· .. 3. Moore CP: Eyelid and nasolacrimal disease, Vet Clin
N Am Equine 8:499, 1992.
Medications: Systemic and topical broad-spec- 4. Samuelson D: Ophthalmic anatomy. In Gelatt KN,
trum antibiotics are used initially pending culture editors: Veterinary ophthalmology, ed 3, Philadel-
and susceptibility of the affected area, and tetanus. phia, 1999, Lippincott, Williams & Wilkins.
prophylaxis should be given. Appropriate antibi- 5. Cooley PL: Normal equine ocular anatomy and eye
otics are continued for 7 days. Nonsteroidal anti- examination, Vet Cli11 N Am Equine Pract 8:427,
inflammatory therapy is necessary for a minimum 1992.
of 3 clays. 6. Moore CP, Constantinescu GM: Surgery of the
other: Cold compresses should be applied post- adnexa, Vet Clin N Am Small Anim Pract 27:1011,
operatively to combat inflammation and edema. 1997.
Protedion: Protective eye cups are recom- 7. Miller TR: Eyelids. In Auer JA, Stick JA, editors: Equin.e
mended to prevent self-trauma.2•3 surgery, ed 2, Philadelphia, 1999, WB Saunders.