
Page 244 - Manual of Equine Field Surgery
P. 244
240 FEMALE UROGENITAL SURGERIES
'
*Ec,,A~~
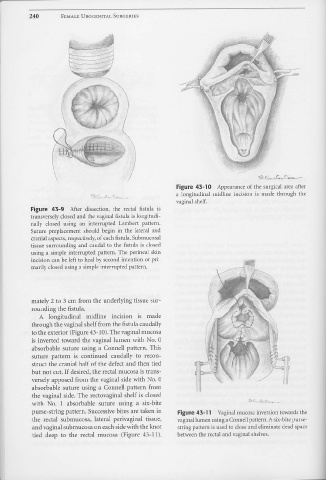
Figure 43-10 Appearance of the surgical area after
a longitudinal rnidline incision is made through the
vaginal shelf.
Figure 43-9 After dissection, the rectal fistula is
transversely closed and the vaginal fistula is longitudi-
nally closed using an interrupted Lembert pattern.
Suture preplacement should begin in the lateral and
cranial aspects, respectively, of each fistula. Submucosal
tissue surrounding and caudal to the fistula is closed
using a simple interrupted pattern. The perineal skin
incision can be left to heal by second intention or pri- I:: ?G:;j
marily closed using a simple interrupted pattern. ------11
mately 2 to 3 cm from the underlying tissue sur-
rounding the fistula.
A longitudinal midline incision is made
through the vaginal shelf from the fistula caudally
to the exterior (Figure 43-10). The vaginal mucosa
is inverted toward the vaginal lumen with No. 0
absorbable suture using a Connell pattern. This
suture pattern is continued caudally to recon- ~,
struct the cranial half of the defect and then tied ~==d 'f
but not cut. If desired, the rectal mucosa is trans-
·~
versely apposed from the vaginal side with No. 0 !~
absorbable suture using a Connell pattern from
the vaginal side. The rectovaginal shelf is closed
with No. 1 absorbable suture using a six-bite
purse-string pattern. Successive bites are taken in Figure 43-11 Vaginal mucosa inversion towards the
the rectal submucosa, lateral perivaginal tissue, vaginal lumen using a Connell pattern. A six-bite purse-
and vaginal submucosa on each side with the knot string pattern is used to close and eliminate dead space
tied deep to the rectal mucosa (Figure 43-11). between the rectal and vaginal shelves .
•