
Page 1246 - Clinical Small Animal Internal Medicine
P. 1246
1184 Section 10 Renal and Genitourinary Disease
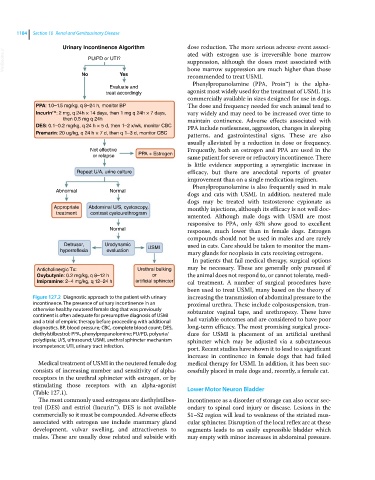
Urinary Incontinence Algorithm dose reduction. The more serious adverse event associ
VetBooks.ir PU/PD or UTI? ated with estrogen use is irreversible bone marrow
suppression, although the doses most associated with
No Yes bone marrow suppression are much higher than those
recommended to treat USMI.
Phenylpropanolamine (PPA, Proin™) is the alpha‐
Evaluate and
treat accordingly agonist most widely used for the treatment of USMI. It is
commercially available in sizes designed for use in dogs.
PPA: 1.0–1.5 mg/kg, q 8–24 h, monitor BP The dose and frequency needed for each animal tend to
Incurin : 2 mg, q 24h × 14 days, then 1 mg q 24h × 7 days, vary widely and may need to be increased over time to
TM
then 0.5 mg q 24h maintain continence. Adverse effects associated with
DES: 0.1–0.2 mg/kg, q 24 h × 5 d, then 1–2 x/wk, monitor CBC PPA include restlessness, aggression, changes in sleeping
Premarin: 20 ug/kg, q 24 h × 7 d, then q 1–3 d, monitor CBC patterns, and gastrointestinal signs. These are also
usually alleviated by a reduction in dose or frequency.
Not effective Frequently, both an estrogen and PPA are used in the
or relapse PPA + Estrogen same patient for severe or refractory incontinence. There
is little evidence supporting a synergistic increase in
Repeat U/A, urine culture efficacy, but there are anecdotal reports of greater
improvement than on a single medication regimen.
Phenylpropanolamine is also frequently used in male
Abnormal Normal
dogs and cats with USMI. In addition, neutered male
dogs may be treated with testosterone cypionate as
Appropriate Abdominal U/S, cystoscopy, monthly injections, although its efficacy is not well doc
treatment contrast cystourethrogram
umented. Although male dogs with USMI are most
responsive to PPA, only 43% show good to excellent
Normal response, much lower than in female dogs. Estrogen
compounds should not be used in males and are rarely
Detrusor, Urodynamic used in cats. Care should be taken to monitor the mam
hyperreflexia evaluation USMI mary glands for neoplasia in cats receiving estrogens.
In patients that fail medical therapy, surgical options
Anticholinergic Tx: Urethral bulking may be necessary. These are generally only pursued if
Oxybutynin: 0.2 mg/kg, q 8–12 h or the animal does not respond to, or cannot tolerate, medi
Imipramine: 2–4 mg/kg, q 12–24 h artificial sphincter cal treatment. A number of surgical procedures have
been used to treat USMI, many based on the theory of
Figure 127.2 Diagnostic approach to the patient with urinary increasing the transmission of abdominal pressure to the
incontinence. The presence of urinary incontinence in an proximal urethra. These include colposuspension, tran
otherwise healthy neutered female dog that was previously sobturator vaginal tape, and urethropexy. These have
continent is often adequate for presumptive diagnosis of USMI
and a trial of empiric therapy before proceeding with additional had variable outcomes and are considered to have poor
diagnostics. BP, blood pressure; CBC, complete blood count; DES, long‐term efficacy. The most promising surgical proce
diethylstilbestrol; PPA, phenylpropanolomine; PU/PD, polyuria/ dure for USMI is placement of an artificial urethral
polydipsia; U/S, ultrasound; USMI, urethral sphincter mechanism sphincter which may be adjusted via a subcutaneous
incompetence; UTI, urinary tract infection. port. Recent studies have shown it to lead to a significant
increase in continence in female dogs that had failed
Medical treatment of USMI in the neutered female dog medical therapy for USMI. In addition, it has been suc
consists of increasing number and sensitivity of alpha‐ cessfully placed in male dogs and, recently, a female cat.
receptors in the urethral sphincter with estrogen, or by
stimulating those receptors with an alpha‐agonist Lower Motor Neuron Bladder
(Table 127.1).
The most commonly used estrogens are diethylstilbes Incontinence as a disorder of storage can also occur sec
trol (DES) and estriol (Incurin™). DES is not available ondary to spinal cord injury or disease. Lesions in the
commercially so it must be compounded. Adverse effects S1–S2 region will lead to weakness of the striated mus
associated with estrogen use include mammary gland cular sphincter. Disruption of the local reflex arc at these
development, vulvar swelling, and attractiveness to segments leads to an easily expressible bladder which
males. These are usually dose related and subside with may empty with minor increases in abdominal pressure.