
Page 114 - Manual of Equine Field Surgery
P. 114
110 LIMB SURGERIES
occurs. This may be related to performing surgery
too soon after diagnostic anesthesia, traumatic
surgical technique, excessive postoperative move-
ment, or incisional site problems. Ideally, surgery
should not be performed for a minimum of
2 weeks after diagnostic anesthesia of the palmar
digital nerve. Surgical technique and handling of
the nerve should be as atraumatic as possible,
and excessive dissection minimized. Adequate
postoperative rest and proper bandaging tech-
niques should be emphasized to the owner. Loss
of the hoof wall as a result of ischemia is a rare
but possible complication. Reasons for its occur-
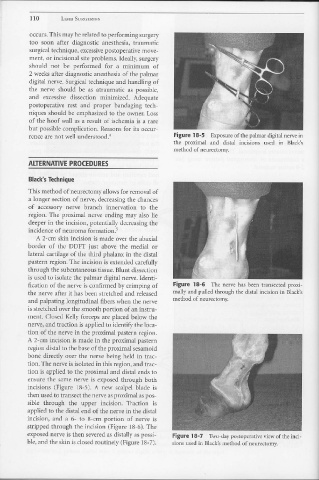
Figure 18-5 Exposure of the palmar digital nerve in
rence are not well understood.4
the proximal and distal incisions t1sed in Black's
method of neurectomy.
ALTERNATIVE PROCEDURES
Black's Technique
This method of neurectomy allows for removal of
a longer section of nerve, decreasing the chances
of accessory nerve branch innervation to the
region. The proximal nerve ending may also lie
deeper ill the incision, potentially decreasing the
incidence of neuroma formation. 5
A 2-cm skin incision is made over the abaxial
border of the DDFT just above the medial or
lateral cartilage of the third phalanx in the distal
pastern region. The incision is extended carefully
through the subcutaneous tissue. Blunt dissection
is used to isolate the palmar digital nerve. Identi-
fication of the nerve is confirmed by crimping of Figure 18-6 The nerve has been transected proxi-
the nerve after it has been stretched and released mally and pulled through the distal incision in Black's
and palpating longitudinal fibers when the nerve method of neurectomy.
is stretched over the smooth portion of an instru-
ment. Closed Kelly forceps are placed below the
nerve, and traction is applied to identify the loca-
tion of the nerve in the proximal pastern region.
A 2-cm incision is made in the proximal pastern
region distal to the base of the proximal sesamoid
bone directly over the nerve being held ill trac-
tion. The nerve is isolated in this region, and trac-
tion is applied to the proximal and distal ends to
ensure the same nerve is exposed through both
incisions (Figure 18-5). A new scalpel blade is
then used to transect the nerve as proximal as pos-
sible through the upper incision. Traction is
applied to the distal end of the nerve in the distal
incision, and a 6- to 8-cm portion of nerve is
stripped through the incision (Figure 18-6). The
exposed nerve is then severed as distally as possi- Figure 18-7 Two-day postoperative view of the inci-
ble, and the skin is closed routinely (Figure 18-7). sions used in Black's method of neurectomy.