
Page 139 - Manual of Equine Field Surgery
P. 139
Tooth Repulsion 135
that will be resistant to future infection. If the plug
does not come out on its own, the horse should
be sedated or anesthetized and the plug removed.
If gauze sponges are used for packing, the sponges
should be replaced every 2 to 3 days.
POSTOPERATIVE CARE
_
..
.... .,._, ,_ .. ~-- ......
~
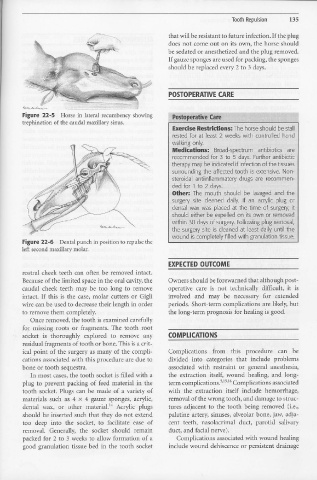
Figure 22-5 Horse in lateral recumbency showing Postoeerative Care
trephination of the caudal maxillary sinus.
Exercise Restridions: The horse should be stall
rested for at least 2 weeks with controlled hand
walking only.
Medications: Broad-spectrum antibiotics are
recommended for 3 to 5 days. Further antibiotic
therapy may be indicated if infection of the tissues
surrounding the affected tooth is extensive. Non-
steroidal antiinflammatory drugs are recommen-
ded for 1 to 2 days.
· Other: The mouth should be lavaged and the
surgery site cleaned daily. If an acrylic plug or
dental wax was placed at the time of surgery, it
should either be expelled on its own or removed
within 30 days of surgery. Following plug removal,
the surgery site is cleaned at least daily until the
wound is completely filled with granulation tissue.
Figure 22-6 Dental punch in position to repulse the
left second maxillary molar.
EXPECTED OUTCOME
rostral cheek teeth can often be removed intact.
Because of the limited space in the oral cavity, the Owners should be forewarned that although post-
caudal cheek teeth may be too long to remove operative care is not technically difficult, it is
intact. If this is the case, molar cutters or Gigli involved and may be necessary for extended
wire can be used to decrease their length in order periods. Short-term complications are likely, but
to remove them completely. the long-term prognosis for healing is good.
Once removed, the tooth is examined carefully
for missing roots or fragments. The tooth root
socket is thoroughly explored to remove any COMPLICATIONS
residual fragments of tooth or bone. This is a crit-
ical point of the surgery as many of the compli- Complications from this procedure can be
cations associated with this procedure are due to divided into categories that include problems
bone or tooth sequestra. associated with restraint or general anesthesia,
In most cases, the tooth socket is filled with a the extraction itself, wound healing, and long-
plug to prevent packing of feed material in the term complications.v":" Complications associated
tooth socket. Plugs can be made of a variety of with the extraction itself include hemorrhage,
materials such as 4 x 4 gauze sponges, acrylic, removal of the wrong tooth, and damage to struc-
dental wax, or other material. L4 Acrylic plugs tures adjacent to the tooth being removed (i.e.,
should be inserted such that they do not extend palatine artery, sinuses, alveolar bone, jaw, adja-
too deep into the socket, to facilitate ease of cent teeth, nasolacrimal duct, parotid salivary
removal. Generally, the socket should remain duct, and facial nerve).
packed for 2 to 3 weeks to allow formation of a Complications associated with wound healing
good granulation tissue bed in the tooth socket include wound dehiscence or persistent drainage