
Page 153 - Manual of Equine Field Surgery
P. 153
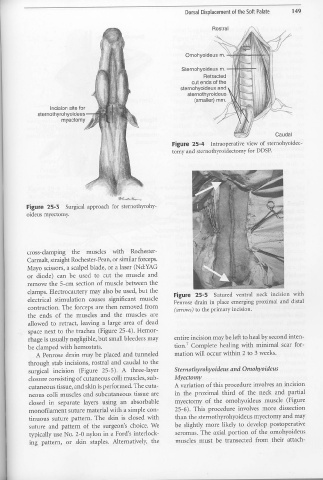
Dorsal Displacement of the Soft Palate 149
Rostral
Omohyoideus m.
Sternohyoideus m. --+~=--....,,.-+-
Retracted
cut ends of the
sternohyoideus and
sternothyroideus
(smaller) mm.
Incision site for
sternothyrohyoideus --T
myectomy
Caudal
Figure 25-4 Intraoperative view of sternohyoidec-
tomy and sternothyroidectomy for DDSP.
~t'....r~..,.
Figure 25-3 Surgical approach for sternothyrohy-
oideus myectomy.
cross-clamping the muscles with Rochester-
Carmalt, straight Rochester-Pean, or similar forceps.
Mayo scissors, a scalpel blade, or a laser (Nd:YAG
or diode) can be used to cut the muscle and
remove the 5-cm section of muscle between the
clamps. Electrocautery may also be used, but the Figure 25-5 Sutured ventral neck incision with
electrical stimulation causes significant muscle Penrose drain in place emerging proximal and distal
contraction. The forceps are then removed from (arrows) to the primary incision.
the ends of the muscles and the muscles are
allowed to retract, leaving a large area of dead
space next to the trachea (Figure 25-4). Hemor-
rhage is usually negligible, but small bleeders may entire incision may be left to heal by second inten-
be clamped with hemostats. tion.' Complete healing with minimal scar for-
A Penrose drain may be placed and tunneled mation will occur within 2 to 3 weeks.
through stab incisions, rostral and caudal to the
surgical incision (Figure 25-5). A three-layer Sternothyrohyoideus and Omohyoideus
closure consisting of cutaneous colli muscles, sub- Myectomy
cutaneous tissue, and skin is performed. The cuta- A variation of this procedure involves an incision
neous colli muscles and subcutaneous tissue are in the proximal third of the neck and partial
closed in separate layers using an absorbable myectomy of the ornohyoideus muscle (Figure
monofilament suture material with a simple con- 25-6). This procedure involves more dissection
tinuous suture pattern. The skin is closed with than the sternothyrohyoideus myectomy and may
suture and pattern of the surgeon's choice. We be slightly more likely to develop postoperative
typically use No. 2-0 nylon in a Ford's interlock- seromas. The axial portion of the ornohyoideus
ing pattern, or skin staples. Alternatively, the muscles must be transected from their attach-
l