
Page 163 - Manual of Equine Field Surgery
P. 163
Modified Forssell's Operation for Cribbing 159
Sternomandibularis m.
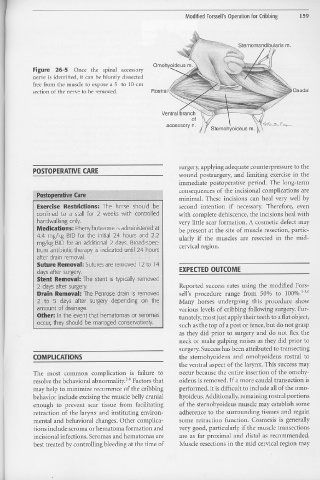
Figure 26-5 Once tl1e spinal accessory
nerve is identified, it can be bluntly dissected
free from the muscle to expose a 5- to 10-cm
section of the nerve to be removed. Rostral . Caudal
Ventral branch
of
accessory n.
Sternohyoideus m.
surgery, .applying adequate counterpressure to the
POSTOPERATIVE CARE
wound postsurgery, and limiting exercise in the
immediate postoperative period. The long-term
«: . '!:t• c consequences of the incisional complications are
os
P t qgera,., 1ve are
minimal. These incisions can heal very well by
Exercise Restridions: The horse should be second intention if necessary, Therefore, even
confined to a stall for 2 weeks with controlled with complete dehiscence, the incisions heal with
handwalking only. very little scar formation. A cosmetic defect may
Medications: Phenylbutazone is administered at be present at the site of muscle resection, partic-
4.4 mg/kg BID for the initial 24 hours and 2.2 ularly if the muscles are resected in the mid-
mg/kg BID for an additional 2 days. Broad-spec- cervical region.
trum antibiotic therapy is indicated until 24 hours
after drain removal.
Suture Removal: Sutures are removed 12 to 14
days after surgery. EXPECTED OUTCOME
Stent Removal: The stent is typically removed
2 days after surgery. Reported success rates using the modified Fors-
Drain Removal: The Penrose drain is removed sell's procedure range from SOo/o to 100%.1-3'6
2 to 5 days after surgery depending on the Many horses undergoing this procedure show
amount of drainage. · various levels of cribbing following st1rgery. For-
Other: In the event that hematomas or seromas tunately, most just apply their teeth to a flat object,
occur, they should be managed conservatively. such as the top of a post or fence, but do not grasp
as they did prior to surgery and do not flex the
neck or make gulping noises as they did prior to
surgery. Success has been attributed to transecting
COMPLICATIONS the sternohyoideus and ornohyoideus rostral to
the ventral aspect of the larynx. This success may
The most common complication is failure to occur because the entire insertion of the omohy-
resolve the behavioral abnormality.i" Factors that oideus is removed. If a more caudal transection is
may help to minimize recurrence of the cribbing performed, it is difficult to include all of the omo-
behavior include excising the muscle belly cranial hyoideus. Additionally, remaining rostral portions
enough to preve11t scar tissue from facilitating of the sternohyoideus muscle may establish some
retraction of the larynx and instituting environ- adherence to the surrounding tissues and regain
mental and behavioral changes. Other complica- some retraction function. Cosmesis is generally
tions include seroma or hematoma formation and very good, particularly if the muscle transections
incisional infections. Seromas and hematomas are are as far proximal and distal as recommended.
best treated by controlling bleeding at the time of Muscle resections in the mid cervical region may
•
•