
Page 243 - Manual of Equine Field Surgery
P. 243
Rectovaginal Fistula Repair 239
\
-
~·
It! . • .;;?":~ - . ,, I
. I"
.
~ ..... ~
'
.. '
j
I
~&-.,~~ ... t.'""""-- ~
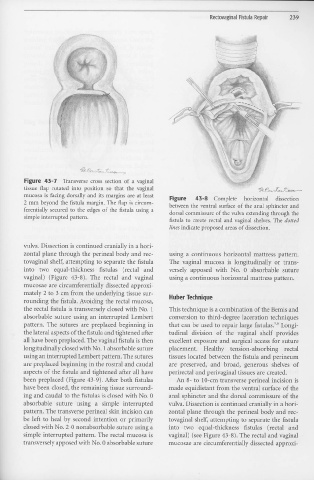
Figure 43- 7 Transverse cross section of a vaginal
tissue flap rotated into position so that the vaginal ~ 0 ..,. ,&,
;,,~-'1')v!l~+./--
mucosa is facing dorsally and its margins are at least Figure 43-8 Complete horizontal dissection
2 mm beyond the fistula margin. The flap is circum- between the ventral surface of the anal sphincter and
ferentially secured to the edges of the fistula using a dorsal commissure of the vulva extending through the
simple interrupted pattern.
fistula to create rectal and vaginal shelves. The dotted
lines indicate proposed areas of dissection.
vulva. Dissection is continued cranially in a hori-
zontal plane through the perineal body and rec- using a continuous horizontal mattress pattern.
tovaginal shelf, attempting to separate the fistula The vaginal mucosa is longitudinally or trans-
into two equal-thickness :fistulas (rectal and versely apposed with No. 0 absorbable suture
vaginal) (Figure 43-8). The rectal and vaginal using a continuous horizontal mattress pattern.
mucosae are circumferentially dissected approxi-
mately 2 to 3 cm from the underlying tissue sur- Huber Technique
rounding the fistula. Avoiding the rectal mucosa,
the rectal :fistula is transversely closed with No. 1 This technique is a combination of the Bemis and
absorbable suture using an interrupted Lembert conversion to third-degree laceration techniques
pattern. The sutures are preplaced beginning iI1 that can be used to repair large fistulas. Longi-
5'6
the lateral aspects of the fistula and tightened after tudinal division of the vaginal shelf provides
all have been preplaced. The vaginal :fistula is then excellent exposure and surgical access for suture
longitudinally closed with No. 1 absorbable suture placement. Healthy tension-absorbing rectal
using an interrupted Lembert pattern. The sutures tissues located between the fistula and perineum
are preplaced beginning in the rostral and caudal are preserved, and broad, generous shelves of
aspects of the :fistula and tightened after all have perirectal and perivaginal tissues are created.
been preplaced (Figure 43-9). After both :fistulas An 8- to 10-cm transverse perinea! incision is
have been closed, the remaining tissue surround- made equidistant from the ventral surface of the
ing and caudal to the fistulas is closed with No. 0 anal sphincter and the dorsal commissure of the
absorbable suture using a simple interrupted vulva. Dissection is continued cranially in a hori-
pattern. The transverse perinea! skin incision can zontal plane through the perineal body and rec-
be left to heal by second intention or primarily tovaginal shelf, attempting to separate the fistula
closed with No. 2-0 nonabsorbable suture using a into two equal-thickness fistulas (rectal and
simple interrupted pattern. The rectal mucosa is vaginal) (see Figure 43-8). The rectal and vaginal
transversely apposed with No. 0 absorbable suture mucosae are circumferentially dissected approxi-