
Page 242 - Manual of Equine Field Surgery
P. 242
238 FEMALE UROGENITAL SURGERIES
A B
Figure 43-4 A, Preplacement of submucosal suture
pattern in a transverse direction beginning in the
corners of the fistula using a simple interrupted pattern.
B, Sagittal cross section of submucosa suture place-
ment. Avoid penetrating the rectal and vaginal
mucosae.
--------·-
.
'
~~"C...;f:'--
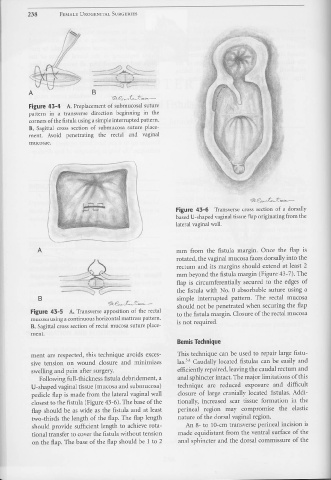
Figure 43-6 Transverse cross section of a dorsally
based U-shaped vaginal tissue flap originating from the
lateral vaginal wall .
. ....__ .
A mm from the fistula margin. Once the flap is
rotated, the vaginal mucosa faces dorsally into the
rectum and its margins should extend at least 2
mm beyond the fistula margin (Figure 43-7). The
flap is circumferentially secured to the edges of
the fistula with No. 0 absorbable suture using a
B simple interrupted pattern. The rectal mucosa
should not be penetrated when securing the flap
Figure 43-5 A, Transverse apposition of the rectal to the fistula margin. Closure of the rectal mucosa
mucosa using a continuous horizontal mattress pattern.
B, Sagittal cross section of rectal mucosa suture place- is not required.
ment.
Bemis Technique
ment are respected, this technique avoids exces- This technique can be used to repair large fistu-
sive tension on wound closure and minimizes las.3'4 Caudally located fistulas can be easily and
swelling and pain after surgery. efficiently repaired, leaving the caudal rectum and
Following full-thickness fistula debridement, a anal sphincter intact. The major limitations of this
U-shaped vaginal tissue (mucosa and submucosa) technique are reduced exposure and difficult
pedicle flap is made from the lateral vaginal wall closure of large cranially located fistulas. Addi-
closest to the fistula (Figure 43-6). The base of the tionally, increased scar tissue formation in the
flap should be as wide as the fistula and at least perineal region may compromise the elastic
two-thirds the length of the flap. The flap length nature of the dorsal vaginal region.
should provide sufficient length to achieve rota- An 8- to 10-cm transverse perineal incision is
tional transfer to cover the fistula without tension made equidistant from the ventral surface of the
on the flap. The base of the flap should be 1 to 2 anal sphincter and the dorsal commissure of the