
Page 237 - Manual of Equine Field Surgery
P. 237
Third-Degree Perinea! Laceration Repair 233
such as dehiscence or fistula formation are
reported to occur in 12°/o to 24o/o of all surgical
repairs.2•4•6•7 Subsequent surgeries are essential
when complications arise to improve the chances
for complete healing. Conception rates are
reported to be 75% to 92% within 1 year after
surgery.2•4•6•7 Third-degree lacerations recur in 5%
to 50°/o of foaling mares due to tl1e inelasticity of
the resultant scar tissue.2-4•6•7
COMPLICATIONS
Suture dehiscence and subsequent fistula devel-
opment are possible. These complications can be
avoided by precise dissection, adequate tissue pur-
chases, and reduced tension on apposed tissues.
Fistula formation may result in failure to conceive
due to endometritis, pneumovagina, or contin-
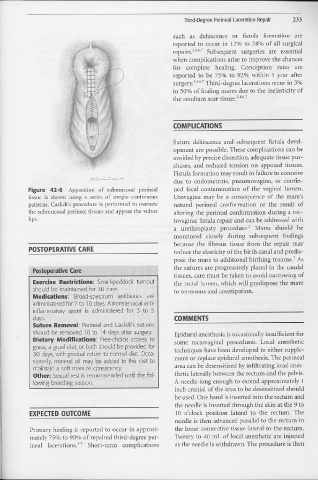
Figure 42-8 Apposition of submucosal perineal ued fecal contamination of the vaginal lumen.
tissue is shown using a series of simple continuous Urovagina may be a consequence of the mare's
patterns. Caslick's procedure is performed to oversew natural perineal conformation or the result of
the submucosal perinea! tissues and appose the vulvar altering the perineal conformation during a rec-
lips. tovaginal fistula repair and can be addressed with
a urethroplasty procedure.2 Mares should be
monitored closely during subsequent foalings
because the fibrous tissue from the repair may
POSTOPERATIVE CARE reduce the elasticity of the birth canal and predis-
7
pose the mare to additional birthing trauma. As
····· Postoperative Care the sutures are progressively placed in the caudal
tissues, care must be taken to avoid narrowing of
Exercise Restridions: Small-paddock turnout the rectal lumen, which will predispose the mare
should be maintained for 30 days. to tenesmus and constipation.
Medications; Broad-spectrum antibiotics are
administered for 7 to l O days. A nonsteroidal anti-
inflammatory agent is administered for 3 to 5
days. COMMENTS
Suture Removal: Perinea! and Caslick's sutures
should be removed l O to 14 days after surgery. Epidural anesthesia is occasionally insufficient for
Dietary Modifications: Free-choice access to some rectovaginal procedures. Local anesthetic
grass, a gruel diet, or both should be provided for techniques have been developed to either supple-
30 days, with gradual return to normal diet. Occa-
sionally, mineral oil may be added to the diet to ment or replace epidural anesthesia. The perineal
maintain a soft manure consistency. area can be desensitized by infiltrating local anes-
Other: Sexual rest is recommended until the fol- thetic laterally between the rectum and the pelvis.
lowing breeding season. A needle long enough to extend approximately 1
inch cranial of the area to be desensitized should
be used. One hand is inserted into the rectum and
the needle is inserted through the skin at the 9 to
EXPECTED OUTCOME 10 o'clock position lateral to the rectum. The
needle is then advanced parallel to the rectum iI1
Primary healing is reported to occur in approxi- the loose connective tissue lateral to the rectum.
mately 75°/o to 90°/o of repaired third-degree per- Twenty to 40 n1L of local anesthetic are injected
inea! lacerations."? Short-term complications as the needle is withdrawn. The procedure is then