
Page 234 - Manual of Equine Field Surgery
P. 234
230 FEMALE UROGENITAL SURGERIES
Cushing or Lembert pattern (Figure 42-4). continuous pattern ending at the center of the
Closure of the rectovaginal shelf and mucosal sur- shelf. The left side is closed in the same manner.
faces should extend to the cutaneous perineum. A Rectal and vaginal mucosa surfaces should not be
Caslick's procedure is then performed to appose penetrated.
the vulvar opening. Perineal body reconstruction begins at the
caudal edge of the newly formed rectovaginal
Semitransverse Closure Technique shelf and is continued caudally. The first suture
Small marker incisions are made at the ventral incorporates the caudal end of the newly formed
aspect of the perineal body along the left and right rectovaginal shelf and the right and left sides of
mucocutaneous junctions"; these markers will be the perineal body. The dorsal portion of the per-
used as the ventrocaudal points of the triangle inea! body is closed first with No. 2 absorbable
used to construct the perineal body. The scar suture using a Cushing pattern. Incorporation of
tissue mucosal junction along the rectovaginal the rectal, vaginal, or anal mucosa should be
shelf is incised longitudinally and divided in its avoided during closure. The remainder of the
entirety. Rectal and vaginal mucosae are under- perineal tissue is closed with No. 2-0 absorbable
mined approximately 7 to 10 cm from the recto- suture using a simple interrupted pattern.
vaginal shelf Beginning approximately 4 cm Caslick's procedure is performed to appose the
cranial to the external anal sphincter, a mucosal perineal skin and vulvar opening.
incision is made from the lateral edge of the rec-
tovaginal shelf ventrocaudally toward the original Two-Stage Repair
marker incision. A triangle-shaped section of
mucosa is excised; the exposed triangular section Aanes Technique
of submucosa will form the perineal body when The vaginal mucosa is inverted into the vaginal
sutured. The center of the rectovaginal shelf is lumen with No. 0 absorbable suture using a
grasped with Allis tissue forceps, pulling the shelf Connell or Lembert pattern. 6•7 This suture pattern
caudally to the cranial border of the proposed is continued caudally to reconstruct the cranial
perinea! body. The final configuration is in the half of the defect and then tied but not cut. Using
shape of a Y, with the base of the Y pointing No. 1 absorbable suture, purse-string sutures are
caudal. Beginning at the deepest corner on the used to close the rectovaginal shelf ( see Figure
right side, the rectovaginal shelf is reconstructed 42-3). Sutures are positioned approximately 1 cm
with No. 2 absorbable suture using a simple apart, avoiding the vaginal and rectal mucosa. If
an excessive amount of tension or dead space is
present, partial tightening of the purse-string
sutures along with sagittally oriented simple inter-
rupted sutures will help obliterate dead space
(Figure 42-5). Once the cranial half of the recto-
vaginal shelf is reconstructed, closure of the
vaginal mucosa is completed, followed by closure
of the remaining caudal half of the rectovaginal
shelf. Optionally, the rectal mucosa may be
inverted into the rectal lumen with No. 2-0
absorbable suture using a Cushing or Lembert
pattern. Closure of the rectovaginal shelf is con-
I tinued to the level of the cutaneous perineum.
Closure of the perineal body is performed 3 to
t 4 weeks after the first surgery if the rectovestibu-
lar shelf is completely healed. If dehiscence occurs
or a fistula is present, the first stage must be
repeated. Local anesthesia of the perineal body or
epidural anesthesia is used. Closure of the per-
inea! body is performed as described in the per-
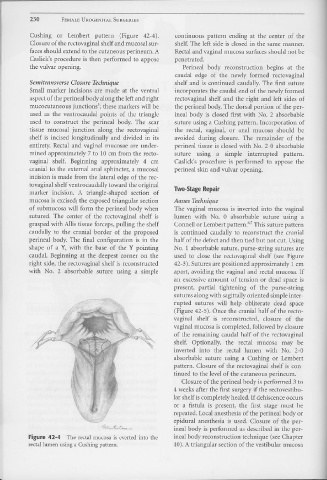
Figure 42-4 The rectal mucosa is everted into tl1e inea! body reconstruction technique ( see Chapter
rectal lumen using a Cushing pattern. 40). A triangular section of the vestibular mucosa