
Page 10 - NYSAGD GP Fall 2018
P. 10
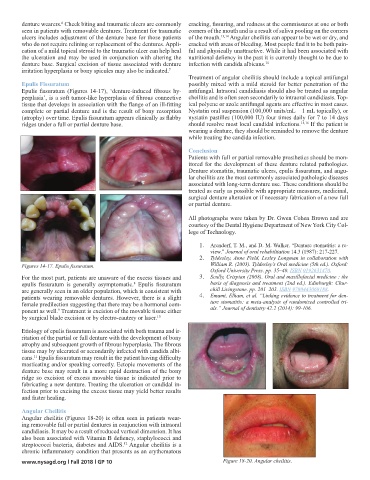
denture wearers. Cheek biting and traumatic ulcers are commonly cracking, fissuring, and redness at the commissures at one or both
6
seen in patients with removable dentures. Treatment for traumatic corners of the mouth and is a result of saliva pooling on the corners
ulcers includes adjustment of the denture base for those patients of the mouth. 13,14 Angular cheilitis can appear to be wet or dry, and
who do not require relining or replacement of the dentures. Appli- cracked with areas of bleeding. Most people find it to be both pain-
cation of a mild topical steroid to the traumatic ulcer can help heal ful and physically unattractive. While it had been associated with
the ulceration and may be used in conjunction with altering the nutritional defiency in the past it is currently thought to be due to
denture base. Surgical excision of tissue associated with denture infection with candida albicans. 15
irritation hyperplasia or bony spicules may also be indicated. 7
Treatment of angular cheilitis should include a topical antifungal
Epulis Fissuratum possibly mixed with a mild steroid for better penetration of the
Epulis fissuratum (Figures 14-17), ‘denture-induced fibrous hy- antifungal. Intraoral candidiasis should also be treated as angular
perplasia’, is a soft tumor-like hyperplasia of fibrous connective cheilitis and is often seen secondarily to intraoral candidiasis. Top-
tissue that develops in association with the flange of an ill-fitting ical polyene or azole antifungal agents are effective in most cases.
complete or partial denture and is the result of bony resorption Nystatin oral suspension (100,000 units/mL – 1 mL topically), or
(atrophy) over time. Epulis fissuratum appears clinically as flabby nystatin pastilles (100,000 IU) four times daily for 7 to 14 days
ridges under a full or partial denture base. should resolve most local candidal infections. 15,16 If the patient is
wearing a denture, they should be reminded to remove the denture
while treating the candida infection.
Conclusion
Patients with full or partial removable prosthetics should be mon-
itored for the development of these denture related pathologies.
Denture stomatitis, traumatic ulcers, epulis fissuratum, and angu-
lar cheilitis are the most commonly associated pathologic diseases
associated with long-term denture use. These conditions should be
treated as early as possible with appropriate measures, medicinal,
surgical denture alteration or if necessary fabrication of a new full
or partial denture.
All photographs were taken by Dr. Gwen Cohen Brown and are
courtesy of the Dental Hygiene Department of New York City Col-
lege of Technology.
1. Arendorf, T. M., and D. M. Walker. “Denture stomatitis: a re-
view.” Journal of oral rehabilitation 14.3 (1987): 217-227.
2. Tyldesley, Anne Field, Lesley Longman in collaboration with
Figures 14-17. Epulis fissuratum. William R. (2003). Tyldesley’s Oral medicine (5th ed.). Oxford:
Oxford University Press. pp. 35–40. ISBN 0192631470.
For the most part, patients are unaware of the excess tissues and 3. Scully, Crispian (2008). Oral and maxillofacial medicine : the
epulis fissuratum is generally asymptomatic. Epulis fissuratum basis of diagnosis and treatment (2nd ed.). Edinburgh: Chur-
8
are generally seen in an older population, which is consistent with chill Livingstone. pp. 201–203. ISBN 9780443068188.
patients wearing removable dentures. However, there is a slight 4. Emami, Elham, et al. “Linking evidence to treatment for den-
female predilection suggesting that there may be a hormonal com- ture stomatitis: a meta-analysis of randomized controlled tri-
ponent as well. Treatment is excision of the movable tissue either als.” Journal of dentistry 42.2 (2014): 99-106.
9
by surgical blade excision or by electro-cautery or laser. 10
Etiology of epulis fissuratum is associated with both trauma and ir-
ritation of the partial or full denture with the development of bony
atrophy and subsequent growth of fibrous hyperplasia. The fibrous
tissue may by ulcerated or secondarily infected with candida albi-
cans. Epulis fissuratum may result in the patient having difficulty
11
masticating and/or speaking correctly. Ectopic movements of the
denture base may result in a more rapid destruction of the bony
ridge so excision of excess movable tissue is indicated prior to
fabricating a new denture. Treating the ulceration or candidal in-
fection prior to excising the excess tissue may yield better results
and faster healing.
Angular Cheilitis
Angular cheilitis (Figures 18-20) is often seen in patients wear-
ing removable full or partial dentures in conjunction with intraoral
candidiasis. It may be a result of reduced vertical dimension. It has
also been associated with Vitamin B defiency, staphylococci and
streptococci bacteria, diabetes and AIDS. Angular cheilitis is a
12
chronic inflammatory condition that presents as an erythematous
www.nysagd.org l Fall 2018 l GP 10 Figure 18-20. Angular cheilitis.