
Page 13 - GP Spring 2020
P. 13
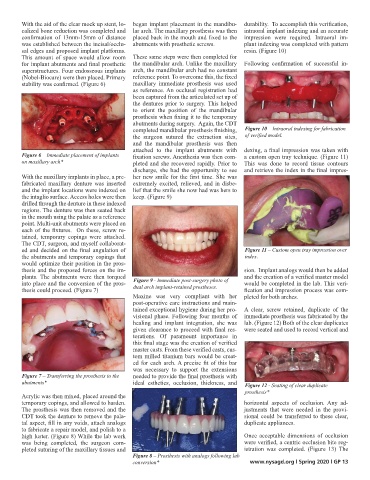
With the aid of the clear mock up stent, lo- began implant placement in the mandibu- durability. To accomplish this verification,
calized bone reduction was completed and lar arch. The maxillary prosthesis was then intraoral implant indexing and an accurate
confirmation of 13mm-15mm of distance placed back in the mouth and fixed to the impression were required. Intraoral im-
was established between the incisal/occlu- abutments with prosthetic screws. plant indexing was completed with pattern
sal edges and proposed implant platforms. resin. (Figure 10)
This amount of space would allow room These same steps were then completed for
for implant abutments and final prosthetic the mandibular arch. Unlike the maxillary Following confirmation of successful in-
superstructures. Four endosseous implants arch, the mandibular arch had no constant
(Nobel-Biocare) were then placed. Primary reference point. To overcome this, the fixed
stability was confirmed. (Figure 6) maxillary immediate prosthesis was used
as reference. An occlusal registration had
been captured from the articulated set up of
the dentures prior to surgery. This helped
to orient the position of the mandibular
prosthesis when fixing it to the temporary
abutments during surgery. Again, the CDT
completed mandibular prosthesis finishing, Figure 10 – Intraoral indexing for fabrication
the surgeon sutured the extraction sites, of verified model.
and the mandibular prosthesis was then
attached to the implant abutments with dexing, a final impression was taken with
Figure 6 – Immediate placement of implants fixation screws. Anesthesia was then com- a custom open tray technique. (Figure 11)
on maxillary arch* pleted and she recovered rapidly. Prior to This was done to record tissue contours
discharge, she had the opportunity to see and retrieve the index in the final impres-
With the maxillary implants in place, a pre- her new smile for the first time. She was
fabricated maxillary denture was inserted extremely excited, relieved, and in disbe-
and the implant locations were indexed on lief that the smile she now had was hers to
the intaglio surface. Access holes were then keep. (Figure 9)
drilled through the denture in these indexed
regions. The denture was then seated back
in the mouth using the palate as a reference
point. Multi-unit abutments were placed on
each of the fixtures. On these, screw re-
tained, temporary copings were attached.
The CDT, surgeon, and myself collaborat-
ed and decided on the final angulation of Figure 11 – Custom open tray impression over
the abutments and temporary copings that index.
would optimize their position in the pros-
thesis and the proposed forces on the im- sion. Implant analogs would then be added
plants. The abutments were then torqued Figure 9 - Immediate post-surgery photo of and the creation of a verified master model
into place and the conversion of the pros- dual arch implant-retained prostheses. would be completed in the lab. This veri-
thesis could proceed. (Figure 7) fication and impression process was com-
Maxine was very compliant with her pleted for both arches.
post-operative care instructions and main-
tained exceptional hygiene during her pro- A clear, screw retained, duplicate of the
visional phase. Following four months of immediate prosthesis was fabricated by the
healing and implant integration, she was lab. (Figure 12) Both of the clear duplicates
given clearance to proceed with final res- were seated and used to record vertical and
torations. Of paramount importance in
this final stage was the creation of verified
master casts. From these verified casts, cus-
tom milled titanium bars would be creat-
ed for each arch. A precise fit of this bar
was necessary to support the extensions
Figure 7 – Transferring the prosthesis to the needed to provide the final prosthesis with
abutments* ideal esthetics, occlusion, thickness, and Figure 12 - Seating of clear duplicate
prosthesis*
Acrylic was then mixed, placed around the
temporary copings, and allowed to harden. horizontal aspects of occlusion. Any ad-
The prosthesis was then removed and the justments that were needed in the provi-
CDT took the denture to remove the pala- sional could be transferred to these clear,
tal aspect, fill in any voids, attach analogs duplicate appliances.
to fabricate a repair model, and polish to a
high luster. (Figure 8) While the lab work Once acceptable dimensions of occlusion
was being completed, the surgeon com- were verified, a centric occlusion bite reg-
pleted suturing of the maxillary tissues and istration was completed. (Figure 13) The
Figure 8 – Prosthesis with analogs following lab
conversion* www.nysagd.org l Spring 2020 l GP 13