
Page 9 - GP Spring 2020
P. 9
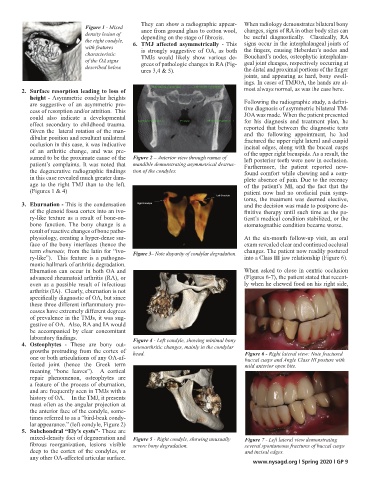
Figure 1 - Mixed They can show a radiographic appear- When radiology demonstrates bilateral bony
density lesion of ance from ground glass to cotton wool, changes, signs of RA in other body sites can
the right condyle, depending on the stage of fibrosis. be useful diagnostically. Classically, RA
with features 6. TMJ affected asymmetrically - This signs occur in the interphalangeal joints of
characteristic is strongly suggestive of OA, as both the fingers, causing Heberden’s nodes and
of the OA signs TMJs would likely show various de- Bouchard’s nodes, osteophytic interphalan-
described below. grees of pathologic changes in RA (Fig- geal joint changes, respectively occurring at
ures 3,4 & 5). the distal and proximal portions of the finger
joints, and appearing as hard, bony swell-
ings. In cases of TMJOA, the hands are al-
2. Surface resorption leading to loss of most always normal, as was the case here.
height - Asymmetric condylar heights
are suggestive of an asymmetric pro- Following the radiographic study, a defini-
cess of resorption and/or attrition. This tive diagnosis of asymmetric bilateral TM-
could also indicate a developmental JOA was made. When the patient presented
for his diagnosis and treatment plan, he
effect secondary to childhood trauma. reported that between the diagnostic tests
Given the lateral rotation of the man- and the following appointment, he had
dibular position and resultant unilateral fractured the upper right lateral and cuspid
occlusion in this case, it was indicative incisal edges, along with the buccal cusps
of an arthritic change, and was pre- of the upper right bicuspids. As a result, the
sumed to be the proximate cause of the Figure 2 – Anterior view through ramus of left posterior teeth were now in occlusion.
patient’s complaints. It was noted that mandible demonstrating asymmetrical destruc- Furthermore, the patient reported new-
the degenerative radiographic findings tion of the condyles. found comfort while chewing and a com-
in this case revealed much greater dam- plete absence of pain. Due to the recency
age to the right TMJ than to the left. of the patient’s MI, and the fact that the
(Figures 1 & 4) patient now had no orofacial pain symp-
toms, the treatment was deemed elective,
3. Eburnation - This is the condensation and the decision was made to postpone de-
of the glenoid fossa cortex into an ivo- finitive therapy until such time as the pa-
ry-like texture as a result of bone-on- tient’s medical condition stabilized, or the
bone function. The bony change is a stomatognathic condition became worse.
result of reactive changes of bone patho-
physiology, creating a hyper-dense sur- At the six-month follow-up visit, an oral
face of the bony interfaces (hence the exam revealed clear and continued occlusal
term eburnate, from the latin for “ivo- Figure 3– Note disparity of condylar degradation. changes. The patient now readily postured
ry-like”). This feature is a pathogno- into a Class III jaw relationship (Figure 6).
monic hallmark of arthritic degradation.
Eburnation can occur in both OA and When asked to close in centric occlusion
advanced rheumatoid arthritis (RA), or (Figures 6-7), the patient stated that recent-
even as a possible result of infectious ly when he chewed food on his right side,
arthritis (IA). Clearly, eburnation is not
specifically diagnostic of OA, but since
these three different inflammatory pro-
cesses have extremely different degrees
of prevalence in the TMJs, it was sug-
gestive of OA. Also, RA and IA would
be accompanied by clear concomitant
laboratory findings. Figure 4 - Left condyle, showing minimal bony
4. Osteophytes - These are bony out- osteoarthritic changes, mainly in the condylar
growths protruding from the cortex of head. Figure 6 - Right lateral view: Note fractured
one or both articulations of any OA-af- buccal cusps and Angle Class III posture with
fected joint (hence the Greek term mild anterior open bite.
meaning “bone leaves”). A cortical
repair phenomenon, osteophytes are
a feature of the process of eburnation,
and are frequently seen in TMJs with a
history of OA. In the TMJ, it presents
most often as the angular projection at
the anterior face of the condyle, some-
times referred to as a “bird-beak condy-
lar appearance.” (left condyle, Figure 2)
5. Subchondral “Ely’s cysts”- These are
mixed-density foci of degeneration and Figure 5 - Right condyle, showing unusually Figure 7 - Left lateral view demonstrating
fibrous reorganization, lesions visible severe bony degradation. several spontaneous fractures of buccal cusps
deep to the cortex of the condyles, or and incisal edges.
any other OA-affected articular surface.
www.nysagd.org l Spring 2020 l GP 9