
Page 6 - GP Spring 2020
P. 6
Case Report: Bridging the Missing Tooth Space
Between an Implant and Natural Tooth
By Philip A. Gentry, DDS, FAGD
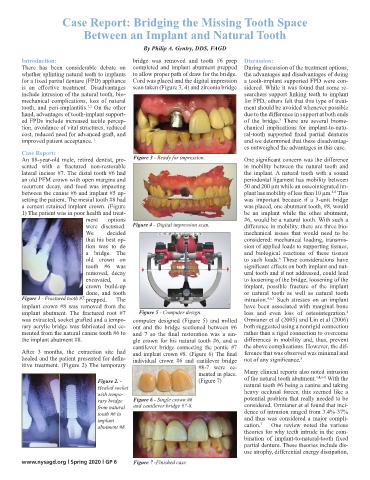
Introduction: bridge was removed and tooth #6 prep Discussion:
There has been considerable debate on completed and implant abutment prepped During discussion of the treatment options,
whether splinting natural teeth to implants to allow proper path of draw for the bridge. the advantages and disadvantages of doing
for a fixed partial denture (FPD) appliance Cord was placed and the digital impression a tooth-implant supported FPD were con-
is an effective treatment. Disadvantages scan taken (Figure 3, 4) and zirconia bridge sidered. While it was found that some re-
include intrusion of the natural tooth, bio- searchers support linking teeth to implant
mechanical complications, loss of natural for FPD, others felt that this type of treat-
1,2
tooth, and peri-implantitis. On the other ment should be avoided whenever possible
hand, advantages of tooth-implant support- due to the difference in support at both ends
ed FPDs include increased tactile percep- of the bridge. There are several biome-
3
tion, avoidance of vital structures, reduced chanical implications for implant-to-natu-
cost, reduced need for advanced graft, and ral-tooth supported fixed partial dentures
improved patient acceptance. 1 and we determined that these disadvantag-
es outweighed the advantages in this case.
Case Report:
An 88-year-old male, retired dentist, pre- Figure 3 - Ready for impression. One significant concern was the difference
sented with a fractured non-restorable in mobility between the natural tooth and
lateral incisor #7. The distal tooth #6 had the implant. A natural tooth with a sound
an old PFM crown with open margins and periodontal ligament has mobility between
recurrent decay, and food was impacting 50 and 200 µm while an osseointegrated im-
between the canine #6 and implant #5 up- plant has mobility of less than 10 µm. This
4-6
setting the patient. The mesial tooth #8 had was important because if a 3-unit bridge
a cement retained implant crown. (Figure was placed, one abutment tooth, #8, would
1) The patient was in poor health and treat- be an implant while the other abutment,
ment options #6, would be a natural tooth. With such a
were discussed. Figure 4 - Digital impression scan. difference in mobility, there are three bio-
We decided mechanical issues that would need to be
that his best op- considered: mechanical loading, transmis-
tion was to do sion of applied loads to supporting tissues,
a bridge. The and biological reactions of these tissues
6
old crown on to such loads. These considerations have
tooth #6 was significant effects on both implant and nat-
removed, decay ural tooth and if not addressed, could lead
excavated, a to loosening of the bridge, loosening of the
crown build-up implant, possible fracture of the implant
done, and tooth or natural tooth as well as natural tooth
Figure 1 - Fractured tooth #7. prepped. The intrusion. 4,6,7 Such stresses on an implant
implant crown #8 was removed from the have been associated with marginal bone
implant abutment. The fractured root #7 Figure 5 - Computer design. loss and even loss of osteointegration.
4
was extracted, socket grafted and a tempo- computer designed (Figure 5) and milled Ormianer et al (2005) and Lin et al (2006)
rary acrylic bridge was fabricated and ce- out and the bridge sectioned between #6 both suggested using a nonrigid connection
mented from the natural canine tooth #6 to and 7 so the final restoration was a sin- rather than a rigid connection to overcome
the implant abutment #8. gle crown for his natural tooth #6, and a differences in mobility and, thus, prevent
cantilever bridge connecting the pontic #7 the above complications. However, the dif-
After 3 months, the extraction site had and implant crown #8. (Figure 6) The final ference that was observed was minimal and
healed and the patient presented for defin- individual crown #6 and cantilever bridge not of any significance.
8
itive treatment. (Figure 2) The temporary #8-7 were ce-
mented in place. Many clinical reports also noted intrusion
Figure 2. - (Figure 7) of the natural tooth abutment. 3,4,6-8 With the
Healed socket natural tooth #6 being a canine and taking
with tempo- heavy occlusal forces, this seemed like a
rary bridge Figure 6 - Single crown #6 potential problem that really needed to be
from natural and cantilever bridge #7-8. considered. Ormianer et al found that inci-
tooth #6 to dence of intrusion ranged from 3.4%-37%
implant and thus was considered a major compli-
7
abutment #8. cation. One review noted the various
theories for why teeth intrude in the com-
bination of implant-to-natural-tooth fixed
partial denture. These theories include dis-
use atrophy, differential energy dissipation,
www.nysagd.org l Spring 2020 l GP 6 Figure 7 -Finished case.