
Page 23 - Avoid Food and Drug Interactions
P. 23
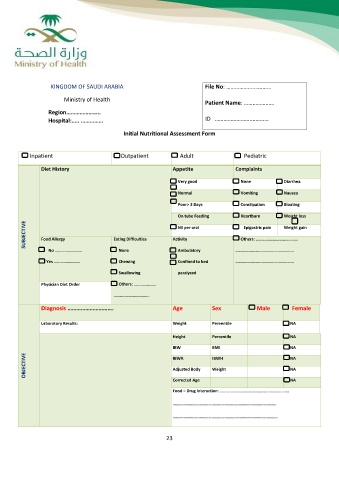
KINGDOM OF SAUDI ARABIA File No: ……………….…………
Ministry of Health Patient Name: …………………
ID ……………………..…….….
Region…………………..
Hospital:….. ……………
Initial Nutritional Assessment Form
Inpatient Outpatient Adult Pediatric
Diet History Appetite Complaints
Very good None Diarrhea
Normal
Poor> 3 Days Vomiting Nausea
On tube Feeding
Nil per oral Constipation Bloating
Activity
Ambulatory Heartburn Weight loss
Confined to bed
SUBJECTIVE paralyzed Epigastric pain Weight gain
Food Allergy Eating Difficulties Others: ……………………….………..
………………………………………………
No ……………………. None ………………………………………………
Yes …………………… Chewing
Swallowing
Physician Diet Order Others: ………….…….
……………………..…….
Diagnosis …………………………. Age Sex Male Female
Laboratory Results: Weight Pereentile NA
Height Percentile NA
IBW BMI NA
OBJECTIVE IBWA IBWH NA
Adjusted Body Weight NA
Corrected Age NA
Food – Drug Interaction: ……………………………………………………….
……………………………………………………………………………………
…………………………………………………………………………………….
23