
Page 327 - Libro 2
P. 327
20 — The Renal Vasculature
307
Interlobular arteries and veins
Arcuate arteries and veins
Interlobar arteries and veins
Nephron
Renal column
Medullary pyramid
Cortex
Renal artery Renal vein
Renal pelvis Renal hilum
Ureter
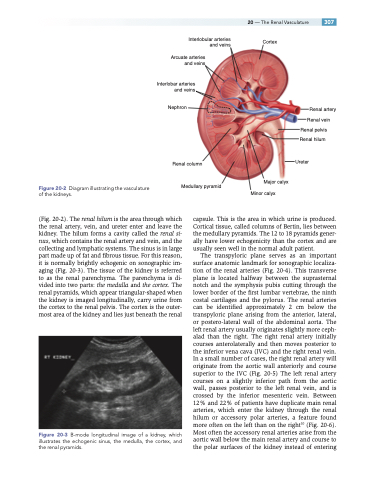
Diagram illustrating the vasculature of the kidneys.
Major calyx Minor calyx
Figure 20-2
(Fig. 20-2). The renal hilum is the area through which the renal artery, vein, and ureter enter and leave the kidney. The hilum forms a cavity called the renal si- nus, which contains the renal artery and vein, and the collecting and lymphatic systems. The sinus is in large part made up of fat and fibrous tissue. For this reason, it is normally brightly echogenic on sonographic im- aging (Fig. 20-3). The tissue of the kidney is referred to as the renal parenchyma. The parenchyma is di- vided into two parts: the medulla and the cortex. The renal pyramids, which appear triangular-shaped when the kidney is imaged longitudinally, carry urine from the cortex to the renal pelvis. The cortex is the outer- most area of the kidney and lies just beneath the renal
Figure 20-3 B-mode longitudinal image of a kidney, which illustrates the echogenic sinus, the medulla, the cortex, and the renal pyramids.
capsule. This is the area in which urine is produced. Cortical tissue, called columns of Bertin, lies between the medullary pyramids. The 12 to 18 pyramids gener- ally have lower echogenicity than the cortex and are usually seen well in the normal adult patient.
The transpyloric plane serves as an important surface anatomic landmark for sonographic localiza- tion of the renal arteries (Fig. 20-4). This transverse plane is located halfway between the suprasternal notch and the symphysis pubis cutting through the lower border of the first lumbar vertebrae, the ninth costal cartilages and the pylorus. The renal arteries can be identified approximately 2 cm below the transpyloric plane arising from the anterior, lateral, or postero-lateral wall of the abdominal aorta. The left renal artery usually originates slightly more ceph- alad than the right. The right renal artery initially courses anterolaterally and then moves posterior to the inferior vena cava (IVC) and the right renal vein. In a small number of cases, the right renal artery will originate from the aortic wall anteriorly and course superior to the IVC (Fig. 20-5) The left renal artery courses on a slightly inferior path from the aortic wall, passes posterior to the left renal vein, and is crossed by the inferior mesenteric vein. Between 12% and 22% of patients have duplicate main renal arteries, which enter the kidney through the renal hilum or accessory polar arteries, a feature found more often on the left than on the right10 (Fig. 20-6). Most often the accessory renal arteries arise from the aortic wall below the main renal artery and course to the polar surfaces of the kidney instead of entering
