
Page 140 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 140
126 SECTION II Autonomic Drugs
Quaternary amines for gastrointestinal and pulmonary applications (peptic disease, COPD):
O
C O
H
H + C 3 7
O C O CH 2 CH 2 N CH 3 C
N
+
O C 3 H 7
OH H C CH 3
3
Propantheline Glycopyrrolate
Tertiary amines for peripheral applications:
O
C H
2 5
CH OH CH 2 CH 3 COCH CH N
2
2
2
C H
2 5
CH C N CH 2 N
O
Tropicamide Dicyclomine
(mydriatric, cycloplegic) (peptic disease, hypermotility)
Quaternary amine for use in asthma: Tertiary amine for Parkinson’s disease:
CH 3 CH 3 N CH 3
S +
O N CH O
C C O
S H O
OH
Tiotropium Benztropine
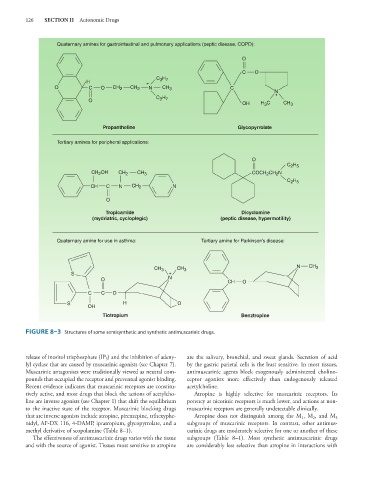
FIGURE 8–3 Structures of some semisynthetic and synthetic antimuscarinic drugs.
release of inositol trisphosphate (IP ) and the inhibition of adeny- are the salivary, bronchial, and sweat glands. Secretion of acid
3
lyl cyclase that are caused by muscarinic agonists (see Chapter 7). by the gastric parietal cells is the least sensitive. In most tissues,
Muscarinic antagonists were traditionally viewed as neutral com- antimuscarinic agents block exogenously administered cholino-
pounds that occupied the receptor and prevented agonist binding. ceptor agonists more effectively than endogenously released
Recent evidence indicates that muscarinic receptors are constitu- acetylcholine.
tively active, and most drugs that block the actions of acetylcho- Atropine is highly selective for muscarinic receptors. Its
line are inverse agonists (see Chapter 1) that shift the equilibrium potency at nicotinic receptors is much lower, and actions at non-
to the inactive state of the receptor. Muscarinic blocking drugs muscarinic receptors are generally undetectable clinically.
that are inverse agonists include atropine, pirenzepine, trihexyphe- Atropine does not distinguish among the M , M , and M
1
2
3
nidyl, AF-DX 116, 4-DAMP, ipratropium, glycopyrrolate, and a subgroups of muscarinic receptors. In contrast, other antimus-
methyl derivative of scopolamine (Table 8–1). carinic drugs are moderately selective for one or another of these
The effectiveness of antimuscarinic drugs varies with the tissue subgroups (Table 8–1). Most synthetic antimuscarinic drugs
and with the source of agonist. Tissues most sensitive to atropine are considerably less selective than atropine in interactions with