
Page 12 - 2021-2022 New Hire Benefits
P. 12
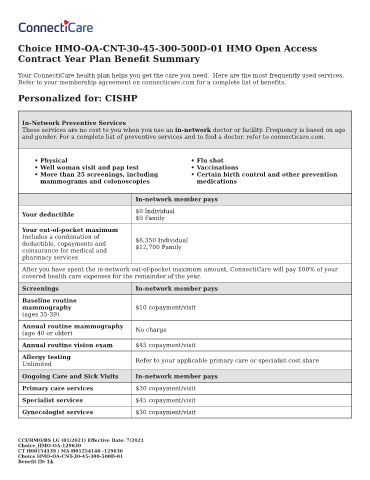
Choice HMO-OA-CNT-30-45-300-500D-01 HMO Open Access
Contract Year Plan Bene t Summary
Your ConnectiCare health plan helps you get the care you need. Here are the most frequently used services.
Refer to your membership agreement on connecticare.com for a complete list of bene ts.
Personalized for: CISHP
In-Network Preventive Services
These services are no cost to you when you use an in-network doctor or facility. Frequency is based on age
and gender. For a complete list of preventive services and to nd a doctor, refer to connecticare.com.
• Physical • Flu shot
• Well woman visit and pap test • Vaccinations
• More than 25 screenings, including • Certain birth control and other prevention
mammograms and colonoscopies medications
In-network member pays
$0 Individual
Your deductible
$0 Family
Your out-of-pocket maximum
Includes a combination of
deductible, copayments and $6,350 Individual
$12,700 Family
coinsurance for medical and
pharmacy services
After you have spent the in-network out-of-pocket maximum amount, ConnectiCare will pay 100% of your
covered health care expenses for the remainder of the year.
Screenings In-network member pays
Baseline routine
mammography $10 copayment/visit
(ages 35-39)
Annual routine mammography No charge
(age 40 or older)
Annual routine vision exam $45 copayment/visit
Allergy testing Refer to your applicable primary care or specialist cost share
Unlimited
Ongoing Care and Sick Visits In-network member pays
Primary care services $30 copayment/visit
Specialist services $45 copayment/visit
Gynecologist services $30 copayment/visit
CCI/HMO/BS LG (01/2021) E ective Date: 7/2021
Choice_HMO-OA-129630
CT H00154139 / MA H01254140 -129630
Choice HMO-OA-CNT-30-45-300-500D-01
Bene t ID: Lk