
Page 13 - 2021-2022 New Hire Benefits
P. 13
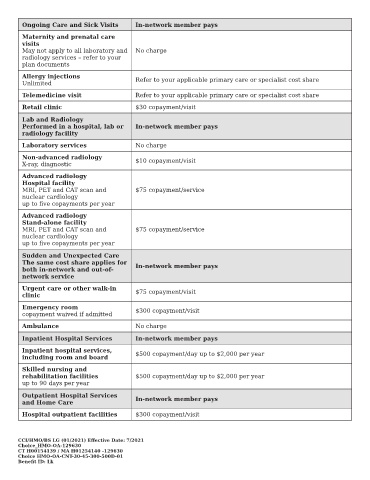
Ongoing Care and Sick Visits In-network member pays
Maternity and prenatal care
visits
May not apply to all laboratory and No charge
radiology services – refer to your
plan documents
Allergy injections Refer to your applicable primary care or specialist cost share
Unlimited
Telemedicine visit Refer to your applicable primary care or specialist cost share
Retail clinic $30 copayment/visit
Lab and Radiology
Performed in a hospital, lab or In-network member pays
radiology facility
Laboratory services No charge
Non-advanced radiology $10 copayment/visit
X-ray, diagnostic
Advanced radiology
Hospital facility
MRI, PET and CAT scan and $75 copayment/service
nuclear cardiology
up to ve copayments per year
Advanced radiology
Stand-alone facility
MRI, PET and CAT scan and $75 copayment/service
nuclear cardiology
up to ve copayments per year
Sudden and Unexpected Care
The same cost share applies for In-network member pays
both in-network and out-of-
network service
Urgent care or other walk-in $75 copayment/visit
clinic
Emergency room $300 copayment/visit
copayment waived if admitted
Ambulance No charge
Inpatient Hospital Services In-network member pays
Inpatient hospital services, $500 copayment/day up to $2,000 per year
including room and board
Skilled nursing and
rehabilitation facilities $500 copayment/day up to $2,000 per year
up to 90 days per year
Outpatient Hospital Services
and Home Care In-network member pays
Hospital outpatient facilities $300 copayment/visit
CCI/HMO/BS LG (01/2021) E ective Date: 7/2021
Choice_HMO-OA-129630
CT H00154139 / MA H01254140 -129630
Choice HMO-OA-CNT-30-45-300-500D-01
Bene t ID: Lk