
Page 16 - 2021-2022 New Hire Benefits
P. 16
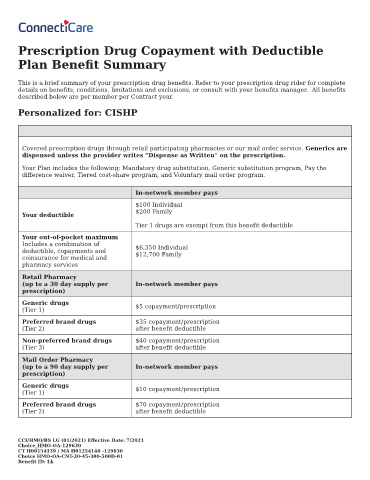
Prescription Drug Copayment with Deductible
Plan Bene t Summary
This is a brief summary of your prescription drug bene ts. Refer to your prescription drug rider for complete
details on bene ts, conditions, limitations and exclusions, or consult with your bene ts manager. All bene ts
described below are per member per Contract year.
Personalized for: CISHP
Covered prescription drugs through retail participating pharmacies or our mail order service. Generics are
dispensed unless the provider writes "Dispense as Written" on the prescription.
Your Plan includes the following: Mandatory drug substitution, Generic substitution program, Pay the
di erence waiver, Tiered cost-share program, and Voluntary mail order program.
In-network member pays
$100 Individual
$200 Family
Your deductible
Tier 1 drugs are exempt from this bene t deductible
Your out-of-pocket maximum
Includes a combination of
deductible, copayments and $6,350 Individual
$12,700 Family
coinsurance for medical and
pharmacy services
Retail Pharmacy
(up to a 30 day supply per In-network member pays
prescription)
Generic drugs
(Tier 1) $5 copayment/prescription
Preferred brand drugs $35 copayment/prescription
(Tier 2) after bene t deductible
Non-preferred brand drugs $40 copayment/prescription
(Tier 3) after bene t deductible
Mail Order Pharmacy
(up to a 90 day supply per In-network member pays
prescription)
Generic drugs $10 copayment/prescription
(Tier 1)
Preferred brand drugs $70 copayment/prescription
(Tier 2) after bene t deductible
CCI/HMO/BS LG (01/2021) E ective Date: 7/2021
Choice_HMO-OA-129630
CT H00154139 / MA H01254140 -129630
Choice HMO-OA-CNT-30-45-300-500D-01
Bene t ID: Lk