
Page 5 - 2022 Drive Open Enrollment Guide - Non Union
P. 5
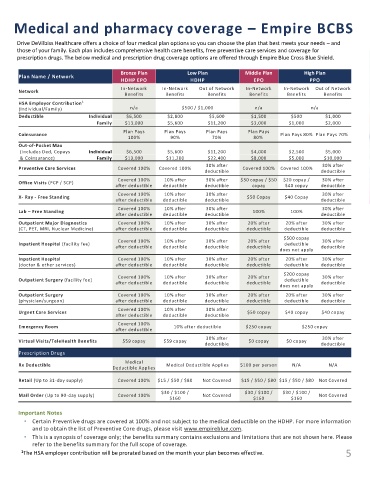
Medical and pharmacy coverage – Empire BCBS
Drive DeVilbiss Healthcare offers a choice of four medical plan options so you can choose the plan that best meets your needs – and
those of your family. Each plan includes comprehensive health care benefits, free preventive care services and coverage for
prescription drugs. The below medical and prescription drug coverage options are offered through Empire Blue Cross Blue Shield.
Bronze Plan Low Plan Middle Plan High Plan
Plan Name / Network
HDHP EPO HDHP EPO PPO
In-Network In-Network Out of Network In-Network In-Network Out of Network
Network
Benefits Benefits Benefits Benefits Benefits Benefits
HSA Employer Contribution 1
(Individual/Family) n/a $500 / $1,000 n/a n/a
Deductible Individual $6,500 $2,800 $5,600 $1,500 $500 $1,000
Family $13,000 $5,600 $11,200 $3,000 $1,000 $2,000
Plan Pays Plan Pays Plan Pays Plan Pays
Coinsurance Plan Pays 80% Plan Pays 70%
100% 90% 70% 80%
Out-of-Pocket Max
(Includes Ded, Copays Individual $6,500 $5,600 $11,200 $4,000 $2,500 $5,000
& Coinsurance) Family $13,000 $11,200 $22,400 $8,000 $5,000 $10,000
30% after 30% after
Preventive Care Services Covered 100% Covered 100% Covered 100% Covered 100%
deductible deductible
Covered 100% 10% after 30% after $30 copay / $50 $20 copay / 30% after
Office Visits (PCP / SCP)
after deductible deductible deductible copay $40 copay deductible
Covered 100% 10% after 30% after 30% after
X- Ray - Free Standing $50 Copay $40 Copay
after deductible deductible deductible deductible
Covered 100% 10% after 30% after 30% after
Lab – Free Standing 100% 100%
after deductible deductible deductible deductible
Outpatient Major Diagnostics Covered 100% 10% after 30% after 20% after 20% after 30% after
(CT, PET, MRI, Nuclear Medicine) after deductible deductible deductible deductible deductible deductible
$500 copay
Covered 100% 10% after 30% after 20% after 30% after
Inpatient Hospital (facility fee) deductible
after deductible deductible deductible deductible deductible
does not apply
Inpatient Hospital Covered 100% 10% after 30% after 20% after 20% after 30% after
(doctor & other services) after deductible deductible deductible deductible deductible deductible
$200 copay
Covered 100% 10% after 30% after 20% after 30% after
Outpatient Surgery (facility fee) deductible
after deductible deductible deductible deductible deductible
does not apply
Outpatient Surgery Covered 100% 10% after 30% after 20% after 20% after 30% after
(physician/surgeon) after deductible deductible deductible deductible deductible deductible
Covered 100% 10% after 30% after
Urgent Care Services $50 copay $40 copay $40 copay
after deductible deductible deductible
Covered 100%
Emergency Room 10% after deductible $250 copay $250 copay
after deductible
30% after 30% after
Virtual Visits/TeleHealth Benefits $59 copay $59 copay $0 copay $0 copay
deductible deductible
Prescription Drugs
Medical
Rx Deductible Medical Deductible Applies $100 per person N/A N/A
Deductible Applies
Retail (Up to 31-day supply) Covered 100% $15 / $50 / $80 Not Covered $15 / $50 / $80 $15 / $50 / $80 Not Covered
$30 / $100 / $30 / $100 / $30 / $100 /
Mail Order (Up to 90-day supply) Covered 100% Not Covered Not Covered
$160 $160 $160
Important Notes
• Certain Preventive drugs are covered at 100% and not subject to the medical deductible on the HDHP. For more information
and to obtain the list of Preventive Core drugs, please visit www.empireblue.com.
• This is a synopsis of coverage only; the benefits summary contains exclusions and limitations that are not shown here. Please
refer to the benefits summary for the full scope of coverage.
1 The HSA employer contribution will be prorated based on the month your plan becomes effective. 5