
Page 7 - 2022 MLB Benefit Guide 08.2022
P. 7
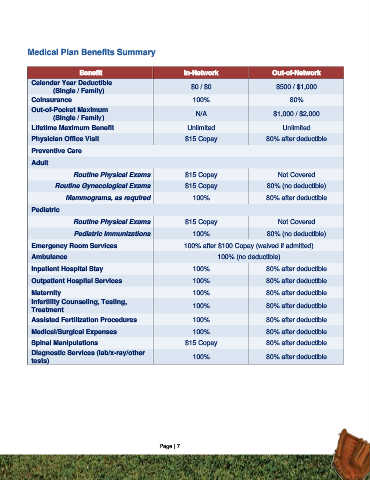
Medical Plan Benefits Summary
Benefit In-Network Out-of-Network
Calendar Year Deductible
(Single / Family) $0 / $0 $500 / $1,000
Coinsurance 100% 80%
Out-of-Pocket Maximum
(Single / Family) N/A $1,000 / $2,000
Lifetime Maximum Benefit Unlimited Unlimited
Physician Office Visit $15 Copay 80% after deductible
Preventive Care
Adult
Routine Physical Exams $15 Copay Not Covered
Routine Gynecological Exams $15 Copay 80% (no deductible)
Mammograms, as required 100% 80% after deductible
Pediatric
Routine Physical Exams $15 Copay Not Covered
Pediatric Immunizations 100% 80% (no deductible)
Emergency Room Services 100% after $100 Copay (waived if admitted)
Ambulance 100% (no deductible)
Inpatient Hospital Stay 100% 80% after deductible
Outpatient Hospital Services 100% 80% after deductible
Maternity 100% 80% after deductible
Infertility Counseling, Testing,
Treatment 100% 80% after deductible
Assisted Fertilization Procedures 100% 80% after deductible
Medical/Surgical Expenses 100% 80% after deductible
Spinal Manipulations $15 Copay 80% after deductible
Diagnostic Services (lab/x-ray/other
tests) 100% 80% after deductible
Page | 7