
Page 6 - 2022 Infoblox Benefits Guide
P. 6
Spending Income Optional
Contents Eligibility Medical Contributions Dental Vision Accounts Protection Benefits Contacts
Plan Comparisons
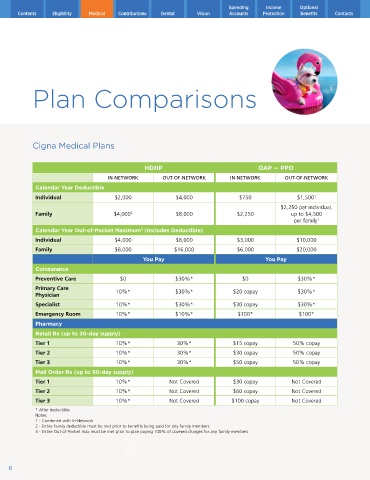
Cigna Medical Plans
HDHP OAP — PPO
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Calendar Year Deductible
Individual $2,000 $4,000 $750 $1,500 1
$2,250 per individual,
Family $4,000 2 $8,000 $2,250 up to $4,500
per family 1
Calendar Year Out-of-Pocket Maximum (Includes Deductible)
3
Individual $4,000 $8,000 $3,000 $10,000
Family $8,000 $16,000 $6,000 $20,000
You Pay You Pay
Coinsurance
Preventive Care $0 $30%* $0 $30%*
Primary Care
Physician 10%* $30%* $20 copay $30%*
Specialist 10%* $30%* $30 copay $30%*
Emergency Room 10%* $10%* $100* $100*
Pharmacy
Retail Rx (up to 30-day supply)
Tier 1 10%* 30%* $15 copay 50% copay
Tier 2 10%* 30%* $30 copay 50% copay
Tier 3 10%* 30%* $50 copay 50% copay
Mail Order Rx (up to 90-day supply)
Tier 1 10%* Not Covered $30 copay Not Covered
Tier 2 10%* Not Covered $60 copay Not Covered
Tier 3 10%* Not Covered $100 copay Not Covered
* After deductible
Notes:
1 - Combined with In-Network
2 - Entire family deductible must be met prior to benefits being paid for any family members
3 - Entire Out-of-Pocket max must be met prior to plan paying 100% of covered charges for any family members
6