
Page 7 - 2022 Infoblox Benefits Guide
P. 7
Spending Income Optional
Contents Eligibility Medical Contributions Dental Vision Accounts Protection Benefits Contacts
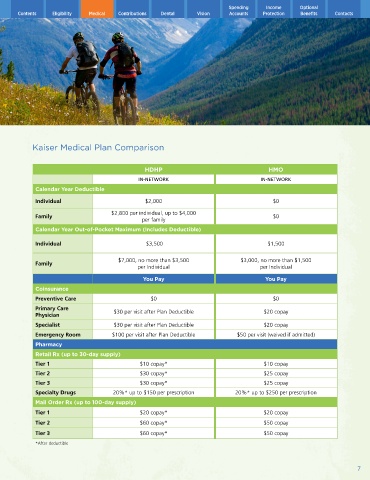
Kaiser Medical Plan Comparison
HDHP HMO
IN-NETWORK IN-NETWORK
Calendar Year Deductible
Individual $2,000 $0
$2,800 per individual, up to $4,000
Family $0
per family
Calendar Year Out-of-Pocket Maximum (Includes Deductible)
Individual $3,500 $1,500
$7,000, no more than $3,500 $3,000, no more than $1,500
Family
per Individual per Individual
You Pay You Pay
Coinsurance
Preventive Care $0 $0
Primary Care
Physician $30 per visit after Plan Deductible $20 copay
Specialist $30 per visit after Plan Deductible $20 copay
Emergency Room $100 per visit after Plan Deductible $50 per visit (waived if admitted)
Pharmacy
Retail Rx (up to 30-day supply)
Tier 1 $10 copay* $10 copay
Tier 2 $30 copay* $25 copay
Tier 3 $30 copay* $25 copay
Specialty Drugs 20%* up to $150 per prescription 20%* up to $250 per prescription
Mail Order Rx (up to 100-day supply)
Tier 1 $20 copay* $20 copay
Tier 2 $60 copay* $50 copay
Tier 3 $60 copay* $50 copay
*After deductible
7