
Page 11 - PriMed 2022 Benefits Guide
P. 11
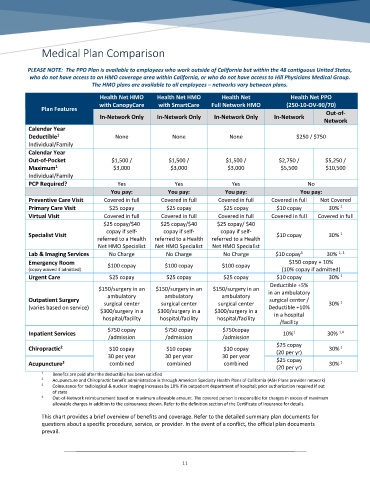
Medical Plan Comparison
PLEASE NOTE: The PPO Plan is available to employees who work outside of California but within the 48 contiguous United States,
who do not have access to an HMO coverage area within California, or who do not have access to Hill Physicians Medical Group.
The HMO plans are available to all employees – networks vary between plans.
Health Net HMO Health Net HMO Health Net Health Net PPO
with CanopyCare with SmartCare Full Network HMO (250-10-OV-90/70)
Plan Features
In-Network Only In-Network Only In-Network Only In-Network Out-of-
Network
Calendar Year
1
Deductible None None None $250 / $750
Individual/Family
Calendar Year
Out-of-Pocket $1,500 / $1,500 / $1,500 / $2,750 / $5,250 /
1
Maximum $3,000 $3,000 $3,000 $5,500 $10,500
Individual/Family
PCP Required? Yes Yes Yes No
You pay: You pay: You pay: You pay:
Preventive Care Visit Covered in full Covered in full Covered in full Covered in full Not Covered
1
Primary Care Visit $25 copay $25 copay $25 copay $10 copay 30%
Virtual Visit Covered in full Covered in full Covered in full Covered in full Covered in full
$25 copay/$40 $25 copay/$40 $25 copay/ $40
copay if self- copay if self- copay if self-
1
Specialist Visit $10 copay 30%
referred to a Health referred to a Health referred to a Health
Net HMO Specialist Net HMO Specialist Net HMO Specialist
3
1, 3
Lab & Imaging Services No Charge No Charge No Charge $10 copay 30%
Emergency Room $100 copay $100 copay $100 copay $150 copay + 10%
(copay waived if admitted) (10% copay if admitted)
1
Urgent Care $25 copay $25 copay $25 copay $10 copay 30%
Deductible +5%
$150/surgery in an $150/surgery in an $150/surgery in an in an ambulatory
ambulatory ambulatory ambulatory
Outpatient Surgery surgical center / 1
surgical center surgical center surgical center 30%
(varies based on service) Deductible +10%
$300/surgery in a $300/surgery in a $300/surgery in a
in a hospital
hospital/facility hospital/facility hospital/facility
/facility
$750 copay $750 copay $750copay
1
1,4
Inpatient Services 10% 30%
/admission /admission /admission
$25 copay
2
1
Chiropractic $10 copay $10 copay $10 copay (20 per yr) 30%
30 per year 30 per year 30 per year
1
Acupuncture 2 combined combined combined $25 copay 30%
(20 per yr)
1 Benefits are paid after the deductible has been satisfied
2 Acupuncture and Chiropractic benefit administration is through American Specialty Health Plans of California (ASH Plans provider network)
3 Coinsurance for radiological & nuclear imaging increases by 10% if in outpatient department of hospital; prior authorization required If out
of state
4 Out-of-Network reimbursement based on maximum allowable amount. The covered person is responsible for charges in excess of maximum
allowable charges in addition to the coinsurance shown. Refer to the definition section of the Certificate of Insurance for details.
This chart provides a brief overview of benefits and coverage. Refer to the detailed summary plan documents for
questions about a specific procedure, service, or provider. In the event of a conflict, the official plan documents
prevail.
11