
Page 15 - McLarty 2017-2018 Benefits Booklet_Finished
P. 15
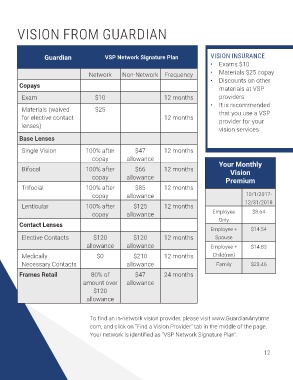
VISION FROM GUARDIAN
Guardian VSP Network Signature Plan VISION INSURANCE
• Exams $10
Network Non-Network Frequency • Materials $25 copay
• Discounts on other
Copays materials at VSP
Exam $10 12 months providers
• It is recommended
Materials (waived $25 that you use a VSP
for elective contact 12 months provider for your
lenses)
vision services
Base Lenses
Single Vision 100% after $47 12 months
copay allowance
Bifocal 100% after $66 12 months Your Monthly
Vision
copay allowance Premium
Trifocial 100% after $85 12 months
copay allowance 10/1/2017-
12/31/2018
Lenticular 100% after $125 12 months
copay allowance Employee $8.64
Only
Contact Lenses
Employee + $14.54
Elective Contacts $120 $120 12 months Spouse
allowance allowance Employee + $14.83
Medically $0 $210 12 months Child(ren)
Necessary Contacts allowance Family $23.46
Frames Retail 80% of $47 24 months
amount over allowance
$120
allowance
To find an in-network vision provider, please visit www.GuardianAnytime.
com, and click on “Find a Vision Provider” tab in the middle of the page.
Your network is identified as “VSP Network Signature Plan”.
12