
Page 6 - REM Medical Solutions - Physicians Guide
P. 6
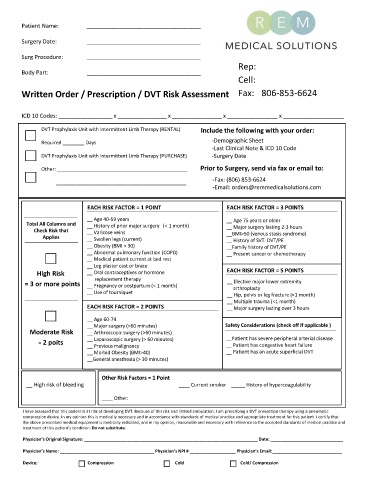
Patient Name: ____________________________________
Surgery Date: ____________________________________
Surg Procedure: ____________________________________
Body Part: ____________________________________
Written Order / Prescription / DVT Risk Assessment 806-853-6624
ICD 10 Codes: _________________ x ________________ x ________________ x ________________ x ___________________
DVT Prophylaxis Unit with Intermittent Limb Therapy (RENTAL) Include the following with your order:
Required ________ Days -Demographic Sheet
-Last Clinical Note & ICD 10 Code
DVT Prophylaxis Unit with Intermittent Limb Therapy (PURCHASE) -Surgery Date
Other: ________________________________________________ Prior to Surgery, send via fax or email to:
________________________________________________ -Fax: (806) 853-6624
-Email: orders@remmedicalsolutions.com
DVT Risk Assesment
EACH RISK FACTOR = 1 POINT EACH RISK FACTOR = 3 POINTS
__ Age 40- 59 years __ Age 75 years or older
Total All Columns and __ History of prior major surgery (< 1 mon th) __ Major surgery lasting 2- 3 hours
Check Risk that __ Varicose veins __BMI>50 (venous stasis syndrome)
Applies __ Swollen legs (current) __ History of SVT. DVT/PE
__ Obesity (BMI > 30) __Family history of DVT/PE
__ Abnormal pulmonary function (COPD) __ Present cancer or chemotherapy
__ Medical patient current at bed rest
__ Leg plaster cast or brace
High Risk __ Oral contraceptives or hormone EACH RISK FACTOR = 5 POINTS
replacement therapy
= 3 or more points __ Pregnancy or postpartum (< 1 month) __ Elective major lower extremity
arthroplasty
__ Use of tourniquet __ Hip, pelvis or leg fracture (<1 month)
__ Multiple trauma (<1 month)
EACH RISK FACTOR = 2 POINTS __ Major surgery lasting over 3 hours
__ Age 60- 74
__ Major surgery (>60 minutes) Safety Considerations (check off if applicable )
Moderate Risk __ Arthroscopic surgery (>60 minutes)
= 2 poits __ Laparoscopic surgery (> 60 minutes) __Patient has severe peripheral arterial disease
__ Previous malignancy __ Patient has congestive heart failure
__ Morbid Obesity (BMI>40) __ Patient has an acute superficial DVT
__General anesthesia (> 30 minutes)
Other Risk Factors = 1 Point
__ High risk of bleeding ____ Current smoker _____ History of hypercoagulability
____ Other:
___________________________________________________________________
I have assessed that this patient is at risk of developing DVT. Because of this risk and limited ambulation, I am prescribing a DVT prevention therapy using a pneumatic
compression device. In my opinion this is medically necessary and in accordance with standards of medical practice and appropriate treatment for this patient. I certify that
the above prescribed medical equipment is medically indicated, and in my opinion, reasonable and necessary with reference to the accepted standards of medical practice and
treatment of this patient’s condition. Do not substitute.
Physician’s Original Signature: ________________________________________________________________________ Date: ______________________________
Physician’s Name: _______________________________________ Physician’s NPI # ___________________ Physician’s Email:_____________________________
Device: Compression Cold Cold/ Compression
