
Page 30 - herina surgery and possible lawsuits
P. 30
Despite sufficient scientific data to support the local anesthesia, large epidemiologic and
nationwide information from databases show high use of spinal anesthesia and low use of
local infiltration anesthesia. [69]
Classical tissue repairs
B ass ini s repair". In 1887 Bassim, the Italian (father of modem herniorrhaphy),
revolutionized the concept of surgical treatment of hennas. He advocated ligation and
resection of the hernial sac followed by opening of the fascia transversalis and than
reconstruction of postenor wall of the inguinal canal by approximating the internal oblique,
transverse abdominus and fascia transversalis "triple layer" to the shelving border of the
inguinal ligament with interrupted sutures with silk, leaving the cord under the external
oblique aponeurosis. His recurrence rate of 3% over a period of 3 years was one tenth of the
failure rates observed during that period. Following Bassim’s original report, numerous
techniques (82 inguinal and 79 femoral repairs) have been described. Most common
modification accepted is not to open fascia transversalis and to suture are placed between
transverse abdominis arch and inguinal ligament, which is now recognized as modified
Bassini’s repair.[23]
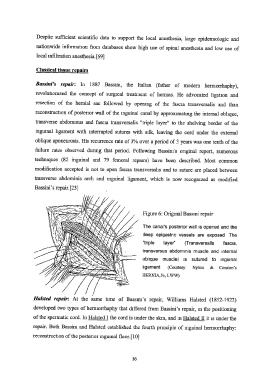
Figure 6: Original Bassmi repair
The canal's posterior wall is opened and the
deep epigastric vessels are exposed The
“triple layer” (Transversalis fascia,
transversus abdominis muscle and internal
oblique muscle) is sutured to inguinal
ligament (Courtesy Nyhus & Condon’s
HERNIA,5e, LWW)
Halsted repair: At the same time of Bassmi’s repair, Williams Halsted (1852-1922)
developed two types of herniorrhaphy that differed from Bassini’s repair, in the positioning
of the spermatic cord. In Halsted I the cord is under the skin, and m Painted TT it is under the
repair. Both Bassim and Halsted established the fourth principle of inguinal herniorrhaphy:
reconstruction of the postenor inguinal floor. [10]
36