
Page 270 - Aida Hovsepian Onboarding
P. 270
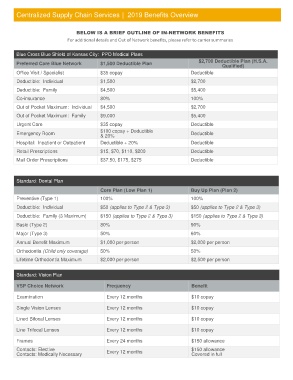
Centralized Supply Chain Services | 2019 Benefits Overview
BELOW IS A BRIEF OUTLINE OF IN-NETWORK BENEFITS
For additional details and Out of Network benefits, please refer to carrier summaries
Blue Cross Blue Shield of Kansas City: PPO Medical Plans
Preferred Care Blue Network $1,500 Deductible Plan $2,700 Deductible Plan (H.S.A.
Qualified)
Office Visit / Specialist $35 copay Deductible
Deductible: Individual $1,500 $2,700
Deductible: Family $4,500 $5,400
Co-insurance 80% 100%
Out of Pocket Maximum: Individual $4,500 $2,700
Out of Pocket Maximum: Family $9,000 $5,400
Urgent Care $35 copay Deductible
Emergency Room $100 copay + Deductible Deductible
& 20%
Hospital: Inpatient or Outpatient Deductible + 20% Deductible
Retail Prescriptions $15, $70, $110, $200 Deductible
Mail Order Prescriptions $37.50, $175, $275 Deductible
Standard: Dental Plan
Core Plan (Low Plan 1) Buy Up Plan (Plan 2)
Preventive (Type 1) 100% 100%
Deductible: Individual $50 (applies to Type 2 & Type 3) $50 (applies to Type 2 & Type 3)
Deductible: Family (3 Maximum) $150 (applies to Type 2 & Type 3) $150 (applies to Type 2 & Type 3)
Basic (Type 2) 80% 90%
Major (Type 3) 50% 60%
Annual Benefit Maximum $1,000 per person $2,000 per person
Orthodontia (Child only coverage) 50% 50%
Lifetime Orthodontia Maximum $2,000 per person $2,500 per person
Standard: Vision Plan
VSP Choice Network Frequency Benefit
Examination Every 12 months $10 copay
Single Vision Lenses Every 12 months $10 copay
Lined Bifocal Lenses Every 12 months $10 copay
Line Trifocal Lenses Every 12 months $10 copay
Frames Every 24 months $150 allowance
Contacts: Elective Every 12 months $150 allowance
Contacts: Medically Necessary Covered in full