
Page 291 - DanielsMarzanoEvidence2020
P. 291
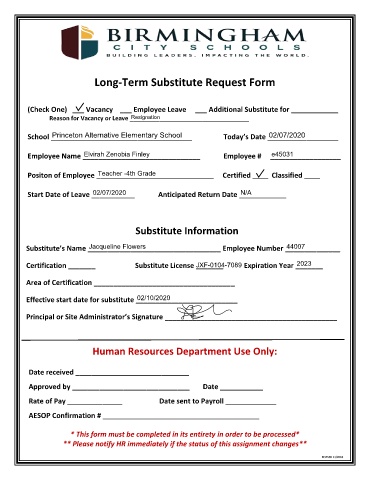
Long-Term Substitute Request Form
(Check One) ___ Vacancy ___ Employee Leave ___ Additional Substitute for ____________
Resignation
Reason for Vacancy or Leave ____________________________________
02/07/2020
Princeton Alternative Elementary School
School ____________________________________ Today’s Date __________________
Elvirah Zenobia Finley
e45031
Employee Name ______________________________ Employee # __________________
Teacher -4th Grade
Positon of Employee ______________________________ Certified ____ Classified ____
02/07/2020
N/A
Start Date of Leave ___________ Anticipated Return Date ____________
Substitute Information
44007
Jacqueline Flowers
Substitute’s Name __________________________________ Employee Number ______________
2023
JXF-0104-7089
Certification _______ Substitute License _______ Expiration Year _______
Area of Certification ____________________________________
02/10/2020
Effective start date for substitute __________________________
Principal or Site Administrator’s Signature ____________________________________________
Human Resources Department Use Only:
Date received _____________________________
Approved by ______________________________ Date ___________
Rate of Pay ______________ Date sent to Payroll _____________
AESOP Confirmation # ________________________________________
* This form must be completed in its entirety in order to be processed*
** Please notify HR immediately if the status of this assignment changes**
REVISED 11/2018