
Page 43 - 2020 Barrister Employee Benefits Book
P. 43
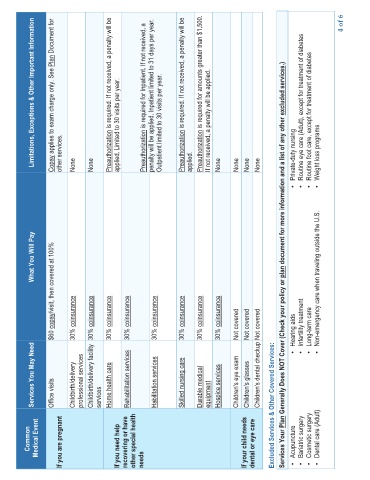
Limitations, Exceptions & Other Important Information
Plan Document for 4 of 6
Copay applies to exam charge only. See other services. None None Preauthorization is required. If not received, a penalty will be applied. Limited to 30 visits per year. Preauthorization is required for Inpatient. If not received, a penalty will be applied. Inpatient limited to 31 days per year. Outpatient limited to 30 visits per year. Preauthorization is required. If not received, a penalty will be applied. Preauthorization is required for amounts greater th
What You Will Pay plan document for more information and a list of any other
copay/visit, then covered at 100% • Non-emergency care when traveling outside the U.S.
$60 coinsurance 30% coinsurance 30% coinsurance 30% coinsurance 30% coinsurance 30% coinsurance 30% coinsurance 30% coinsurance 30% Not covered Not covered Not covered Plan Generally Does NOT Cover (Check your policy or • Hearing aids • Infertility treatment • Long-term care
Services You May Need Office visits Childbirth/delivery professional services Childbirth/delivery facility services Home health care Rehabilitation services Habilitation services Skilled nursing care Durable medical equipment Hospice services Children's eye exam Children's glasses Children's dental checkup Excluded Services & Other Covered Services:
Common Medical Event If you are pregnant If you need help recovering or have other special health needs If your child needs dental or eye care Services Your • Acupuncture • Bariatric surgery • Cosmetic surgery • Dental care (Adult)