
Page 19 - NYMets_2018_Benefits_Guide
P. 19
BACK TO
HOME
PLATE
at-bat: vision benefits
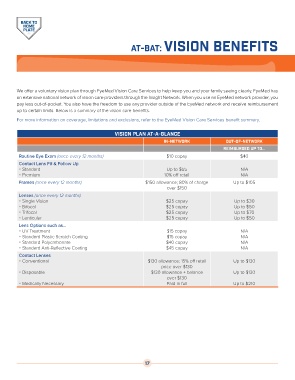
We offer a voluntary vision plan through EyeMed Vision Care Services to help keep you and your family seeing clearly. EyeMed has
an extensive national network of vision care providers through the Insight Network. When you use an EyeMed network provider, you
pay less out-of-pocket. You also have the freedom to use any provider outside of the EyeMed network and receive reimbursement
up to certain limits. Below is a summary of the vision care benefits.
For more information on coverage, limitations and exclusions, refer to the EyeMed Vision Care Services benefit summary.
Vision Plan at-a-glance
in-network Out-of-network
Reimbursed up to...
Routine Eye Exam (once every 12 months) $10 copay $40
Contact Lens Fit & Follow Up
Standard Up to $55 N/A
Premium 10% off retail N/A
Frames (once every 12 months) $150 allowance; 80% of charge Up to $105
over $150
Lenses (once every 12 months)
Single Vision $25 copay Up to $30
Bifocal $25 copay Up to $50
Trifocal $25 copay Up to $70
Lenticular $25 copay Up to $50
Lens Options such as...
UV Treatment $15 copay N/A
Standard Plastic Scratch Coating $15 copay N/A
Standard Polycarbonate $40 copay N/A
Standard Anti-Reflective Coating $45 copay N/A
Contact Lenses
Conventional $130 allowance; 15% off retail Up to $130
price over $130
Disposable $130 allowance + balance Up to $130
over $130
Medically Necessary Paid in full Up to $210
17