
Page 28 - WestCalcasieuCameron2017
P. 28
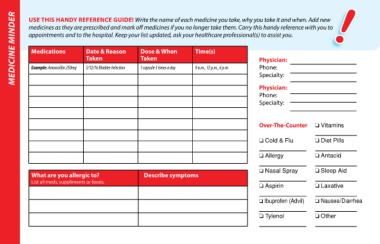
MEDICINE MINDER USE THIS HANDY REFERENCE GUIDE! Write the name of each medicine you take, why you take it and when. Add new My Next Appointment My Next Appointment QUESTIONS FOR MY DOCTOR: APPOINTMENT KEEPER
medicines as they are prescribed and mark off medicines if you no longer take them. Carry this handy reference with you to
appointments and to the hospital. Keep your list updated, ask your healthcare professional(s) to assist you.
Date ____________Time__________
Date ____________Time__________
Time(s)
Date & Reason
Medications
Dose & When
Dr. Name ______________________
Dr. Name ______________________
Taken
Taken
Physician:
Specialty ______________________
Specialty ______________________
Phone:
9 a.m., 12 p.m., 6 p.m.
1 capsule 3 times a day
5/12/16 Bladder Infection
Example: Amoxicillin 250mg
Specialty:
Physician: Address _______________________ Address _______________________
Dr. Ph. # _______________________
Dr. Ph. # _______________________
Phone:
Specialty: Reason for appointment Reason for appointment
_______________________________ _______________________________
Over-The-Counter o Vitamins Questions for my appointment Questions for my appointment
Check any of the boxes below and write notes to Check any of the boxes below and write notes to
o Cold & Flu o Diet Pills remember what to discuss with your doctor. remember what to discuss with your doctor.
I have questions about: I have questions about:
o Allergy o Antacid r My medicines r My medicines
______________________________ ______________________________
o Nasal Spray o Sleep Aid
What are you allergic to? Describe symptoms r My test results r My test results
List all meds, suppliments or foods. ______________________________ ______________________________
o Aspirin o Laxative r My pain r My pain
______________________________ ______________________________
o Ibuprofen (Advil) o Nausea/Diarrhea r Feeling stressed r Feeling stressed
______________________________ ______________________________
o Tylenol o Other r Other questions or concerns r Other questions or concerns
______________________________ ______________________________
27 28