
Page 9 - 2019 Sharks Benefits V6.1
P. 9
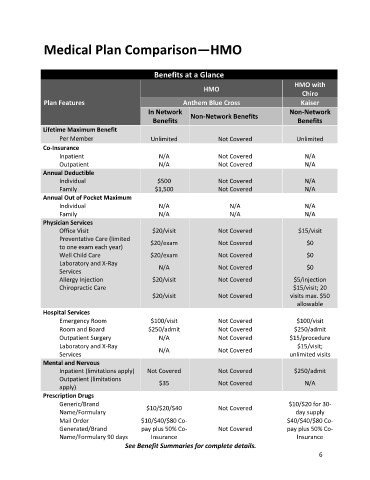
Medical Plan Comparison—HMO
Benefits at a Glance
HMO with
HMO
Chiro
Plan Features Anthem Blue Cross Kaiser
In Network Non-Network
Non-Network Benefits
Benefits Benefits
Lifetime Maximum Benefit
Per Member Unlimited Not Covered Unlimited
Co-Insurance
Inpatient N/A Not Covered N/A
Outpatient N/A Not Covered N/A
Annual Deductible
Individual $500 Not Covered N/A
Family $1,500 Not Covered N/A
Annual Out of Pocket Maximum
Individual N/A N/A N/A
Family N/A N/A N/A
Physician Services
Office Visit $20/visit Not Covered $15/visit
Preventative Care (limited $20/exam Not Covered $0
to one exam each year)
Well Child Care $20/exam Not Covered $0
Laboratory and X-Ray N/A Not Covered $0
Services
Allergy Injection $20/visit Not Covered $5/injection
Chiropractic Care $15/visit; 20
$20/visit Not Covered visits max. $50
allowable
Hospital Services
Emergency Room $100/visit Not Covered $100/visit
Room and Board $250/admit Not Covered $250/admit
Outpatient Surgery N/A Not Covered $15/procedure
Laboratory and X-Ray N/A Not Covered $15/visit;
Services unlimited visits
Mental and Nervous
Inpatient (limitations apply) Not Covered Not Covered $250/admit
Outpatient (limitations $35 Not Covered N/A
apply)
Prescription Drugs
Generic/Brand $10/$20 for 30-
Name/Formulary $10/$20/$40 Not Covered day supply
Mail Order $10/$40/$80 Co- $40/$40/$80 Co-
Generated/Brand pay plus 50% Co- Not Covered pay plus 50% Co-
Name/Formulary 90 days Insurance Insurance
See Benefit Summaries for complete details.
6